

xxx
-
Posts
697 -
Joined
-
Last visited
-
Days Won
88
Posts posted by xxx
-
-
Hey Greeneyes,
I'm not a physician so I don't diagnose and I do not prescribe. If you're looking for information on CH, I'll tell you what I do or what's been reported in the online survey of CHers taking the anti-inflammatory regimen... A headache lasting 30 minutes to an hour does not fit the ICH description for short-lasting unilateral neuralgiform headache with conjunctival injection and tearing (SUNCT), or short-lasting unilateral neuralgiform headache with cranial autonomic features (SUNA). That said, you could have both CH and SUNA so I give your neurologist high marks in trying to diagnose and find an effective treatment for your headaches. There are a few clinical reports/case studies indicating Lamotrigine has been found effective in treating SUNA. See the following link: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4812802/
I tend to be a pragmatist when it comes to treating headaches. In other words, I'm all about if its not broken and working... don't try to fix it! To that end, unless your neurologist told you to stop taking the vitamin D3 regimen and verapamil, OR you're a crusader rabbit and want to find out if Lamotrigine really works to prevent your headache so you stopped taking them on your own... then have at it! We'll never know unless we try... If not, I would jump back into the anti-inflammatory regimen starting with a couple days of vitamin D3 loading doses at 50,000 IU/day along with the rest of this regimen. I'd also start a short 3 to 4 day course of Benadryl (Diphenhydramine HCL) at 25 mg every four hours and 50 mg at bed time. I see no contraindications with Lamotrigine If this stops your headaches or significantly reduces their frequency and severity... then you decide which treatment rout to follow.
Some additional thoughts... You should have been given a Patient Information Sheet with the Lamotrigine. Read it carefully, particularly for signs of allergic reactions.
For reference, when I say "I would try" or take something... I'm saying I've tried it several times and found it effective... To that end, the recurrence of CH symptoms after stopping the vitamin D3 are very common for ECHers in cycle and all CCHers. Tried that too... In fact I intentionally stop taking the anti-inflammatory regimen several times a year to evaluate different dosing schema and other aids like taking Benadryl (Diphenhydramine HCL) to see how fast I get back to a CH pain free state.
Hope this helps...
Take care and please keep us posted.
V/R, Batch
-
Steve,
Please believe me I know how you feel having broken the code so to speak with Claritin. I'm all about if it works, don't screw with it... I would suggest if you haven't already done so, is to get your wife started on the anti-inflammatory regimen. Like you, I have a wonderful supporter who has stood by me and my CH for nearly 24 years. I got her started on this regimen a little over a month after I started it in October of 2010. She had been a migraineur for more than 20 years at that point with migraines hitting for 3 to 5 days a month like clockwork. She hasn't had a single migraine since. She's now 80 and has more energy, getup and go than she did at 60. I'd like to keep her around for a lot longer and the anti-inflammatory regimen appears to be making that happen. At ~ 55 cents a day, it has become a very effective form of health insurance.
We both go in for our annual physicals on the same day and our PCP tells us the same thing. He says to the two of us, "Your labs look great, but your 25(OH)D is elevated... as usual. However as your serum calcium and PTH are well within the normal reference range, I guess you know what you're doing." Neither of us take any prescription medications.
Take care and please keep us posted.
V/R, Batch
-
Hey Ceyron,
We know what you're going through and most of us old timers like CHfather have the T-Shirts and coffee mugs from cluster headache conferences over the years to prove it. He's given you an excellent suggestion on using a freshly charged oxygen cylinder. It's also possible you're having a CGRP cascade triggered by an allergic reaction. When this happens, none of the standard CH interventions work effectively including oxygen.
CHers are typically dehydrated so be sure to drink at least 2.5 liters of water a day. It also helps if you drink a glass of ice water with lots of ice through a straw at the first sign of an approaching CH. Drinking the ice water this way results in a mini brain freeze that chills the hard pallet and Sphenopalatine ganglia located in the back of the nasal cavity to trigger vasoconstriction, one of the key elements responsible for aborting CH.
I've also sent you a PM that you'll need to discuss with your PCP or neurologist as it's very likely you're also vitamin D3 insufficient/deficient. You can download a copy of the anti-inflammatory regimen CH preventative treatment protocol at the following link at the VitaminDWiki web site. It will explain all this and more.
http://www.vitamindwiki.com/tiki-download_wiki_attachment.php?attId=7708
Take care and please keep us posted.
V/R, Batch
-
 1
1
-
-
Hey Steve,
Thanks for the reply and Jon, thanks for the kind words. Like you, I've had plenty of first-hand experience with Benadryl getting my CH back under control with the anti-inflammatory regimen...
Steve, have you downloaded a copy of the latest version of the anti-inflammatory regimen? It contains a major section on the vitamin D3 loading schedules and allergies with the need for a first-generation antihistamine.
An allergic reaction occurs when enough allergens reach a threshold and trigger mast cells to degranulate releasing histamine and a lot of other neuropeptides. The histamine, in turn, triggers neurons to express and release CGRP. If there's a lot of histamine, it triggers a major release of CGRP that turn around and trigger mast cells to release even more histamine. This becomes a circular chemical chain reaction causing a CGRP cascade. When this happens, none of the traditional CH interventions including vitamin D3 and oxygen will be effective. This circular chemical chain reaction continues until one or more of the reactants are consumed at which point the reaction stops and so does the CH... for now... As luck would have it our bodies recharge the mast cells with more histamine and neurons with the building blocks for more CGRP in roughly one or two hours which means the circular chain reactions is primed and ready to go again enabling the CH beast to jump ugly... Sound familiar?
This is where the antihistamine comes into play. By blocking the H1 histamine receptors the antihistamine helps prevent the expression and release of CGRP and this enables vitamin D3 to do its thing to further down-regulate CGRP production and in the process prevent our CH.
If you've been without Claritin for more than 24 hours, the allergens that triggered the initial allergy may have dissipated sufficiently... In any event, I'd keep the Claritin handy as we're surrounded by allergens 7X24.
Take care and please keep us posted on your use of Claritin while taking the anti-inflammatory regimen.
V/R, Batch
Edited to add: Be sure to thank your wife for suggesting the Claritin. Tell her you love her and that her hair or shoes look nice... Wives like to hear things like this. We're usually in such a foul mood during a CH bout that wives keep their distance once they know we're doing something about the CH... Who knows... You might get lucky...
-
1
-
-
Hey Steve,
One question and some comments... When you started the anti-inflammatory regimen, did you also start the 12-Day vitamin D3 loading schedule at 50,000 IU/day for 12 days?
Regarding taking Claritin (Loratadine)... Good move... I've been suggesting a first-generation antihistamine like Benadryl (DIphenhydramine HCL) as it passes through the blood brain barrier to block H1 histamine receptors on neuronal genes throughout the brain and in particular, the trigeminal ganglia where the neurons have a relatively high density of GCRP expressing genes. Blocking the H1 histamine receptors on trigeminal ganglia neurons inhibits the expression and release of Calcitonin Gene-Related Peptides (CGRP), the neuropeptides responsible for neurogenic inflammation and the pain we know as CH.
Claritin (Loratanine) is a second-generation (Less Drowsy) antihistamine that works to block H1 histamine receptors in the periphery and is less able to pass through the blood brain barrier (making it a less drowsy antihistamine). It is also ranked as the least potent of the second-generation antihistamines.
In researching H1 histamine receptors I've found them located in all the major body tissue and cell types. The following BioGPS Gene Atlas for the HRH1 H1 Histamine receptor gene illustrates its relative density across several tissue and cell types.

What the above chart is telling us is there are H1 histamine receptors on neuron genes and other cell types throughout the body that are capable of expressing and releasing CGRP. Your report of Claritin (Loratadine) providing CH relief is a new and welcome data point in our fight to control CH. Benadryl (Diphenhydramine HCL) also works to block H1 histamine receptors on neuron genes and other cells throughout the periphery as well as neurons throughout the brain.
It's also important to note that the genetically active Vitamin D3 metabolite 1,25(OH)2D3 attaches to vitamin D3 receptors (VDR) on neuron genes throughout the brain and trigeminal ganglia and acts through genetic expression to down-regulate the expression and release of CGRP. Accordingly, Vitamin D3 and antihistamines provide a synergistic effect in reducing the expression and release of CGRP... and in the process, help prevent CH. There's a complete section on first-generation antihistamines in the anti-inflammatory regimen CH preventative treatment protocol I had posted 21 Jan 2017 at the VitaminDWiki website at the following link:
http://www.vitamindwiki.com/tiki-download_wiki_attachment.php?attId=7708
I'll be changing the Benadryl (Diphenhydramine HCL) dosing schedule in the next release of this treatment protocol scheduled for Jan of 2018. In the mean time we've found that 25 mg of Benadryl (Diphenhydramine HCL) taken every 4 hours throughout the day and 50 mg at bedtime provides the best protection throughout the day and at night while sleeping against CH while taking the anti-inflammatory regimen. Just be careful and not drive after taking Benadryl (Diphenhydramine HCL) as it will make you drowsy,
Hope this helps and thanks for the feedback. Take care.
V/R, Batch
-
Hey Gail,
Pull down a copy of the anti-inflammatory regimen with 10,000 IU/day vitamin D3 from the following link and read through it. If it looks to your liking, share a copy with your primary care physician when you ask for the lab test of your serum 25(OH)D. Please let me know if you have questions.
http://www.vitamindwiki.com/tiki-download_wiki_attachment.php?attId=7708
Take care and please keep us posted.
V/R, Batch
-
No studies listed in clinicaltrials.gov for Gliacin... There were a handful of studies on Boswellia Serrata, the primary ingredient in Gliacin, but none done on headaches..
V/R, Batch
-
Primrose,
Got it and thanks for the kind words. You have my reply in your PM InBox. Please discuss it with your PCP or neurologist.
Take care and hugs,
V/R, Batch
-
Hey Primrose,
Dallas Denny, CHfather and Spiney have given you some great suggestions that should help to control your CH. I'm particularly interested in your case as you also have episodic migraines with aura. My wife was a migraineur for over 20 years with bouts hitting monthly for 3 to 5 days like clockwork until she started the anti-inflammatory regimen in December of 2010. She hasn't had a migraine since. I've sent you a PM with information to discuss with your PCP or neurologist.
Take care and please keep us posted.
V/R, Batch
-
Hey Atama,
CHfather was spot on suggesting you contact the staff at OUCH-uk. Their Hot Line number is 01646 651 979. You can also go to their website at: https://ouchuk.org/
Ask them to email you a copy of the NHS Home Oxygen Order Form (HOOF), fill out your part and have your PCP or neurologist sign, Keep a copy... This bbn is not accepting attachments for some reason so I can't attach the HOOF at this time. However, if you'll shoot me a PM with your email address, I'll send you a copy.
Check your PM InBox. I've sent you some additional info to discuss with your PCP.
Take care,
V/R, Batch
-
Awesome...
-
1
-
-
Hey MoxieGirl,
Howzit in jolly old England? Howz the head? Long time no hear... Try pasting your link then replace the "." with the word "dot" with the explanation to readers to copy the link, replace the word "dot" with a period then place in their browser. For example, http://isdotgd/clustervitd
Copy this link then replace the word "dot" between "is" and "gd" with a period then past in your browser.
You may also see a black banner come up when you paste a link with "Remove the Link" and a button to do so. Readers will still need to paste the link in their browser,
Take care,
V/R, Batch
-
Hey Ddove,
Good question on the Q Collar. Before venturing an answer if it would help reduce or prevent CH while sleeping, I'll offer the following. The pathogenesis of cluster headache is a complex, multivariate sequence of physiological events that have yet to be fully understood and described by the experts. That the standards of care recommended preventative treatments used by neurologists and headache specialists experienced in treating patients with CH haven't changed in over 20 years gives proof that CH pathogenesis remains a mystery to modern medical science.
Busting and vitamin D3 therapy are the two most promising methods of controlling CH available to us today. Big Pharma is betting hundreds of millions of dollars on the use of monoclonal antibodies with an apatite for calcitonin gene-related peptides (CGRP) as a possible preventative, but they are still years away from an FDA approved biological preventative for CH. Even if they do make it to market, their expense may be prohibitive for many CHers.
It's sites like CB and CH.com that have provided a forum for thousands of CHers to share experiences on what works and what doesn't when it comes to controlling CH that have given us the most useful information. As an example, as cluster headaches are most frequent while sleeping, many of us have found sleeping in a recliner with head elevated at least 6 inches above the heart helps reduce the frequency of CH while sleeping. The physiology behind this is simple. When we sleep, and in particular deep sleep, our respiration rate and heart beat are at their lowest. Blood oxygen levels drop and CO2 levels rise. This creates a perfect storm for CHers so we get hit more frequently.
Elevating the head above the heart means the heart must work harder to pump blood to the brain. This requires more work, burns more fuel and consumes more oxygen... so we breath a little faster sleeping this way. That extra breathing means we ventilate the lungs more, maintain a higher level of blood oxygenation and a lower level of blood CO2.
Back to your question on the Q Collar. It was patterned after the woodpecker's capacity to avoid brain damage wile pecking for food. The principle used here with the Q Collar is to partially block the venous blood flow leaving the brain increasing the volume of blood in the brain to act as "bubble wrap" as the inventor claims, to prevent the brain from sloshing around inside the skull reducing concussion damage while playing football or hockey.
So how would this work while sleeping... My guess is it's going to be a wash or double edged sword. On one hand the Q Collar slows the flow of blood through the brain, as that increases the blood CO2 content and lowers the oxygen content, the brain stem life support functions would signal an increase in respiration. That's the good part. However as the Q Collar physically restricts the flow of blood through the brain, all the house cleaning functions that need to be done while in deep sleep are slowed down. That's the bad part.
That makes the short answer... Wait until the Q Collar hits the market, buy one and see if it's effective in preventing CH or reducing the frequency of CH while sleeping.
Take care and please let us know if the Q Collar helps prevent CH while sleeping.
V/R, Batch
-
1
-
-
Have your husband drink a big glass of ice water... preferably through a straw, The goal of the ice water is to create a mini brain freeze. Chilling the hard pallet chills the sphenopalatine gangia on both sides of the nasal cavity. As the sphenopalatine gangia are connected directly to the trigeminal ganglia where the CH pain originates this chilling triggers the vasoconstriction that is part of the cluster headache abort mechanism. Your husband should be drinking 2.5 liters of water a day.
The reason oxygen therapy and energy drinks are not effective is your husband is either suffering from an allergic reaction or a low grade infection. Both make nearly all the classic CH interventions ineffective.
If I suspect an allergic reaction, and they can be subclinical, i.e., no outward or obvious symptoms, I take Benadryl (Diphenhydramine HCL), 25 mg every four hours during the day and 50 mg before bed. Diphenhydramine is a first generation antihistamine that crosses the blood brain barrier to block H1 histamine receptors on neurons throughout the brain and in particular neurons within the trigeminal ganglia.
An allergic reaction triggers mast cells to dump a flood of histamine and other proinflammatory agents into the surrounding tissues and blood stream. This flood of histamine in turn, triggers neurons throughout the brain to release calcitonin gene-related peptid (CGRP), Substance P (SP) and vasoactive intestinal peptide (VIP). CGRP is the nasty peptide that triggers neurogenic inflammation and the pain we know as cluster headache. CGRP, SP and VIP also trigger mast cells to dump more histamine. This creates a circular chain reaction that continues until one or more of the reactants are consumed at which point the chain reaction and cluster headache pain ends... for now...
Pick up some Benadryl (Diphenhydramine HCL) asap this morning when the nearest supermarket opens. In the mean time, have you husband drink the ice water then try the oxygen therapy.
I've left you a PM in your mail box with information to discuss with your husband's PCP or neurologist, To read it, click on the envelop icon on the right side of the blue border at the top of this page.
Take care and please keep us posted.
V/R, Batch
-
Hey Doug,
You've got the Michigan Headache & Neurological Institute (MHNI) 47 minutes away in Ann Arbor, MI. This is one of the top headache centers in the US with a medical staff of experts in treating patients with primary headaches. It might be worth giving them a call.
It appears Dr. Joel R. Saper is accepting cluster headache patients episodic and chronic for studies of a new intervention, likely one of the mAbs tested earlier on migraineurs.
Take care,
V/R, Batch
-
1
-
-
Hey All,
Thank the money grubbers at photobucket for the missing photos of the Redneck Reservoir Bag. Here they are courtesy of imgur. I used white electrician's tape to make the gas tight seals around the Coke bottle and oxygen tubing. You can see the Duck Tape that seals the open end of the kitchen trash bag. You can use a box cutter to cut the bottom off a plastic Coke bottle. This will become your mouthpiece. Remember to keep the bottle top.
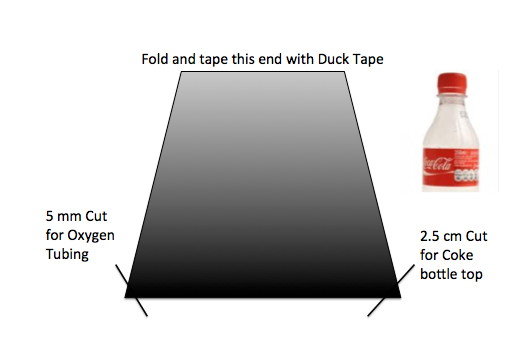



These things are amazing. I have a $500 oxygen demand valve and the Redneck Reservoir bag has zero resistance during inhale... Not so for the oxygen demand valve.
You construct the Redneck Reservoir from a clean Kitchen Trash bag. Start by cutting the oxygen tubing from the mask end of an old disposable oxygen mask. Insert the cut end through the small hole cut in the corner of the closed end of the trash bag and tape with electrician's tape. Make sure the bottle cap is on the Coke bottle and screwed on to prevent any loss of oxygen. Insert the Coke bottle through the hole cut in the other corner from the inside of the back and tape with electrician's tape for a gas tight seal as illustrated in the photo. Put a strip of tape around the middle of the bottle. This becomes your handle. When the oxygen tubing and Coke bottle have been sealed, place the open end of the trash bag on the kitchen counter and use some masking tape at both ends of the opening to hold the open end straight. Fold the open end of the trash bag over at least an inch then seal with a strip of Duck tape for a gas tight seal.
To prepare the Redneck Reservoir for use, connect the oxygen tubing to the barb fitting on your oxygen regulator and make sure the Coke bottle cap is on securely. Open the supply valve on the oxygen cylinder then set the flow rate for 5 to 7 liters/minute until the Redneck Reservoir bag in almost full, then turn off the cylinder supply valve. Check for leaks. You can patch them with the electrician's tape. Your Redneck Reservoir bag is ready to rock n roll...
The procedure for use of the Redneck Reservoir bag is relatively simple... Edited to add... Drink an 8 oz glass of cold ice water before starting this procedure. It helps to drink it rapidly through a straw so you get a mini brain freeze. If there's no decrease in the pain intensity by the 4th to 5th complete hyperventilation cycle or 4 to 5 minutes, drink another 4 to 6 oz of water.
When you've hyperventilated for 30 seconds (ten complete cycles) per the procedures below, unscrew the bottle cap as you wheeze for three seconds, then place the bottle to your lips and inhale oxygen from the reservoir bag rapidly until your lungs are full. Replace the bottle cap asap after inhaling while holding the lungful of oxygen for 30 seconds. When the 30 seconds is up, hyperventilate for another 30 second then repeat the procedure above.
A kitchen trash bag should hold 35 to 40 liters of oxygen so there's more than enough to abort your CH if you use the procedure properly.
Rose, meditation is good during oxygen therapy... and it is best done after hyperventilating with room air as fast as you can for 30 seconds then inhale a lungful of 100% oxygen and hold it for 30 seconds... This is where you meditate....
Yes... you might get a little dizzy... I do on occasion... usually after too many Rum & Cokes... That said, I've never passed out hyperventilating with room air or the oxygen demand valve even though I wished that would happen to escape the pain... It never did/does...
At the end of the 30 seconds holding the lungful of oxygen, exhale with a crunch then do another 30 seconds of hyperventilating with room air. The exhale part of this procedure is important. Exhale rapidly until it feels like your lungs are empty... They're not. At this point you do the abdominal crunch and hold the abdominal crunch and chest squeeze until your exhaled breath makes a wheezing sound for a second then throw your shoulders back and inhale as deeply from the diaphragm as fast as possible then repeat the exhalation with a crunch in one fluid motion. Ten of these complete cycles in 30 seconds should start to push your body into respiratory alkalosis... (Remember the movie "The Andromeda Strain") On the tenth exhalation, hold the squeeze/crunch until your breath makes a wheezing sound for at least 3 seconds... or until you stop wheezing... This will squeeze out another half to full liter of exhaled breath that's highest in CO2 content.
You'll know you're doing this procedure correctly when you feel a slight tingling or prickling on your face, lips, hands, lower legs and feet. This is called paresthesia. You may even feel a slight chill across your back after inhaling the lungful of oxygen and holding it as the capillaries in your skin constrict forcing the blood deeper and allowing your skin to cool. Guess what??? the same thing is happening to the capillaries in and around your trigeminal ganglia where the CH pain is originating... The vasoconstriction is part of the abort mechanism that stops the CH pain and ends the CH attack.
Rose, if you sing the 'Hallelujah Chorus' from Handel's Messiah at Christmas, you have the breath control to use this method of oxygen therapy as there are several places where you need to inhale a lungful of air in less than a second in order to maintain the tempo...
This procedure is not for Bo Peep, but rather for the Wolf who Huffs and Puffs to blow down the pig's house of sticks... In short you huff and puff like a big dog if you're doing this oxygen therapy procedure properly... The meditation comes while holding the lungful of oxygen for 30 seconds... If you're good at this and you will be with a little practice while pain free before your next hit, you'll feel the CH pain start to drain away on the 4th or 5th cycle...
Why hyperventilate during oxygen therapy? The answer is simple once you understand a little about respiratory physiology... For starters, hyperventilation means ventilating the lungs more and faster than normal. What this does is blow off CO2 faster than your body generates it through normal metabolism.
Once you've reduced the CO2 content of your blood, a few things happen... Less CO2 dissolved in the blood means less acid as CO2 dissolves in water to make carbonic acid... that also means the blood becomes more alkaline (the opposite of acid) and this elevates blood pH - a measure of acidity. The elevated pH and lack of CO2 are detected by chemical receptors in the aortic arch and brain. These chemical receptors in turn signal the lungs to slow the respiration rate, the heart to beat more slowly and capillaries throughout the body to constrict (narrow). All this happens to slow the flow of blood to the lungs in order to allow the CO2 level to rise back to normal...
However, as we are intentionally hyperventilating, the lungs keep pumping out more CO2 and the pH goes even higher until we inhale the lungful of 100% oxygen. At this point the elevated pH causes blood hemoglobin to dump CO2 rapidly as it passes through the lungs. The elevated pH also cause blood hemoglobin to have a greater affinity for oxygen so the blood hemoglobin uploads more oxygen than normal creating a hyper-oxygenated blood flow to the brain.
The low CO2 and elevated pH cause capillaries in and around the trigeminal ganglia to constrict. This vasoconstriction coupled with the hyper-oxygenated blood flow is the basic mechanism that aborts CH. If you follow this explanation this far you'll see that it is impossible to pass out while hyperventilating... Your squash (brain) is being loaded with more oxygen than normal and this will keep you wide awake...
What happens after the CH abort? Simple... we start breathing normally and this allows the CO2 levels to rise and the oxygen levels to drop back to normal... All this happens within a minute or two after you stop hyperventilating...
There's one more thing to remember... Oxygen therapy is only an abortive and not a preventative.... Accordingly, your next CH will usually hit right on schedule so you'll need to go though all this again. Some CHers complain when the pain free period ends and that this method of procedure isn't worth the effort... To that I say, balderdash! Seven minutes is the average abort time using this method of oxygen therapy. When you consider the average CH attack lasts anywhere from 30 to 90 minutes... 23 to 83 minutes of pain free time is a very good deal compared to the alternative...
Rose, check you PM inbox. I've left you some additional information to discuss with your PCP or neurologist. You'll find my PM by clicking on the envelop icon in the blue border at the top right corner of this page.
Hope all this helps.
Take care and please keep us posted.
V/R, Batch
-
3
-
-
Most of us old timers are all about educating neurologists about CH... The sad fact is CH is so rare, most neurologist have never treated a patient suffering from CH, let alone have a CHer present with an actual attack... Dr. Todd Rozen did a survey of CHers then added the insight that from his perspective as a seasoned headache specialist having worked out of the top neurological headache institutes and centers, that most neurologists have never treated a patient with CH during their entire career in neurology...
The path of least resistance is usually the best course of action. Take a copy of the anti-inflammatory regimen CH preventative treatment protocol to your PCP and ask for the 25(OH)D lab test. It's a very safe bet your results will come back < 30 ng/mL and for sure < 40 ng/mL. Ask for the Rx for oxygen therapy. The script should read "Oxygen therapy at 15 to 25 liters/minute with a non-rebreathing oxygen mask as an abortive for cluster headache." If I'm correct, pick up the needed supplements and get started. When your appointment comes up with the neurologist in October... you'll have something new to talk about.
Please let us know when you do start this regimen as there can be a few bumps in the road that are easily taken care of if we know you've hit one.
Take care and please keep us posted.
V/R, Batch
-
1
-
-
Awitcher,
Great question and the short answer is Yes. Oxygen therapy, if properly administered can stop a CH hitting while sleeping all the way up to a Kip-9 on the 10-Point Headache Pain Scale. Once a CH has risen to a Kip-10, we're all along for some heavy sledding as very little works to abort CH at this pain level.
You need to understand that oxygen therapy, even administered properly, is still just an abortive and not a preventative... That means your next regularly scheduled CH attack will hit anyway. This can be frustrating until you realize when used properly, oxygen therapy can abort a CH in an average of 7 minutes... When you consider left untreated, a CH can last 30 to 90 minutes... That makes avoiding 23 to 83 minutes of needless CH pain a very good deal...
The better solution is to see your PCP for the 25(OH)D lab test. 25(OH)D is the first metabolite of vitamin D3 that's used to measure its status. It turns out that CHers with active bouts of CH are vitamin D3 deficient or insufficient, a serum 25(OH)D concentration less than 30 ng/mL... As CHers, we need to keep our 25(OH)D serum concentration up around 80 ng/mL in order to keep us CH pain free or significantly reduce the frequency, severity and duration of our CH.
The following chart illustrates the normal distribution curve of baseline 25(OH)D lab results taken before start of the anti-inflammatory regimen with 10,000 IU/day vitamin D3.
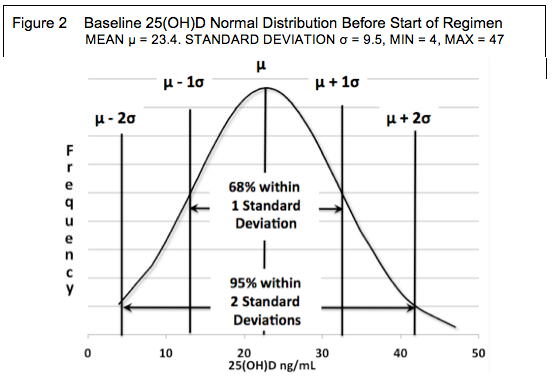
You can download a pdf copy of the anti-inflammatory regimen CH preventative treatment protocol at the following link. Henry Lahore posted this treatment protocol for me on 21 January, 2017. As of this morning, readers at the VitaminDWiki website have downloaded 3295 copies of this treatment protocol
http://www.vitamindwiki.com/tiki-download_wiki_attachment.php?attId=7708
Take care and please keep us posted.
V/R, Batch
-
1
-
-
Hey CHsuckedmylifeaway,
I've sent you a message with some additional information. To read it, click on the envelope icon in the top right blue border at the top of this page. Nerve blocks can bring wonderful relief from the CH pain. However, as they are only providing symptomatic relief and not addressing the underlying causes of CH, they don't last... unless you are episodic and your cycle was ending anyway.
Take care and please keep us posted.
V/R, Batch
-
Hey Greeneyes,
Sorry your neurologist is such a dud... He should have prescribed oxygen... and hyperventilating is helpful in holding the CH pain level down as it elevates your systemic pH making it more alkaline which triggers vasoconstriction.
It's normal for the anti-inflammatory regimen to cause changes in CH patterns until it kicks in for a pain free response. A few CHers have reported switch hitting on the opposite side so nothing new there. That the overall intensity is down is a clear indication you're building your 25(OH)D reserves so a significant response or a pain free response is near. Remember to drink lots of water and if you feel a hit coming on, guzzle a glass of ice water through a straw until it feels like a brain freeze.
Are you still taking the Benadryl (Diphenhydramine HCL)? If not, I've found 25 mg every six hours can work wonders in combating allergic reactions. These can be subcliinical, i.e., no outward or obvious symptoms but the allergic reaction is still there pumping out histamine that makes nearly all CH prevents ineffective.
Take care and please keep us posted.
V/R, Batch
-
Woo Hoo!!! I'll block out the dates as soon as they're available...
V/R, Batch
-
Good points Jon... except I would take it a step further and make an anonymous call to the city health department and report the problem... Raw sewage fumes are a very real health hazard!
V/R, Batch
-
3
-
-
Hey Greeneyes,
As you appear to be responding to this regimen, I would continue the accelerated Vitamin D3 loading schedule at 50,000 IU/day vitamin D3 for another four to five days along with the rest of the anti-inflammatory regimen. This is a safe and effective way of elevating your serum 25(OH)D up near 80 ng/mL where at least 83% of CHers experience a significant drop in the frequency of their CH or a complete cessation of CH.
Poping and chewing the 50,000 IU of vitamin D3 softgels between your back teeth and swirling the contents under your tongue for 5 minutes without swallowing will help in absorption... I do this frequently during my 25(OH)D burn down tests where I stop taking vitamin D3 until my CH return...
I'm a chronic CHer and take an average of 15,000 to 20,000 IU/day vitamin D3 along with the rest of the anti-inflammatory regimen. I've also maintained an average 25(OH)D serum concentration around 140 ng/mL for the last three years. Yes, I know that is above 100 ng/nL.. I also know that the 25(OH)D lab test results are a very poor indicator of vitamin D3 intoxication/toxicity... If we were to equate a high serum concentration of 25(OH)D to vitamin D3 toxicity, there are several RCTs indicating the concentration would be well North of 200 ng/mL.
My PCP is comfortable with my 25(OH)D being this high (It's been over 167 ng/mL) as he has a copy of the anti-inflammatory regimen treatment protocol so knows as long as my serum calcium stays within its normal reference range... and it has... there's no real issue with vitamin D3 toxicity.
As the CH beast is still jumping ugly after a week of 50,000 IU/day vitamin D3, I would start a week to 10 day course of Benadryl (Diphenhydramine HCL) at 25 mg/day... If there's no joy at this dose and the CH beast is still jumping ugly, bump it to 50 mg/day.
Take care and please keep us posted.
V/R, Batch
-
1
-
-
Hey Scubasteb,
If you run into problems following CHfather's excellent suggestion for cash and carry medical oxygen, don't be afraid to buy welder's 02... I understand your concern about cleanliness of welder's O2 cylinders. In reality, this particular issue becomes a mute point when you understand the differences in fill procedures for both industrial and medical oxygen. If you look at the FDA's Compressed Medical Gases Guideline issued under 21 CFR 10.90, the single biggest difference in O2 cylinder fill facility procedures for medical oxygen is a sniff of smell test of cylinder contents before filling. See:
https://www.fda.gov/drugs/guidancecomplianceregulatoryinformation/guidances/ucm124716.htm
As a Director at O.U.C.H. and co-author on a patent for the demand valve method of oxygen therapy as a rapid and reliable CH abortive, I had the opportunity to visit a few medical and industrial oxygen cylinder fill facilities. As the above FDA procedures are not mandatory, most fill facilities use a vent - 2 second fill - vent, then fill sequence for both medical and industrial oxygen cylinders on a multi cylinder fill manifold... In short, I never saw anyone actually smell the contents of an incoming medical oxygen cylinder prior to filling... They all get the same external visual inspection of the cylinder and fill fittings prior to filling.
Nearly all of these fill facilities use the same piping and fill manifold systems for both medical and industrial oxygen cylinders and all use oxygen coming from the same liquid oxygen storage tanks and evaporators for both medical and industrial oxygen. The only differences is the signage :
I've used welder's oxygen from the same welding supply outlet for the last 7 years and never had any problems. I've used the same Flotec InGage 0-60 liter/minute oxygen regulator with a 10-micron sintered metal inlet filter. Once you buy the initial cylinder and that usually comes to $250 to $300 for an M-Size 3995 liter cylinder, you drop it off when empty and pick up a freshly charged cylinder for around $35.
Since I developed the anti-inflammatory regimen with 10,000 IU/day vitamin D3 in October of 2010, my usage of oxygen as a CH abortive has all but stopped completely. I'm on my second M-Size oxygen cylinders since then and as my home is located in deep woods with lots of logging equipment, I actually do my own welding and brazing.
Scan the following following QR code with your smart phone and it will download a pdf copy of the latest Anti-Inflammatory Regimen CH preventative treatment protocol to your phone. The QR Scanner app is free. It takes less than 10 seconds to download and install.

Take care and please keep us posted.
V/R Batch
SUNA and CLUSTERS
in General Board
Posted
Hey Greeneyes,
My hat is off to you and damn the torpedoes full speed ahead.. My wife thinks I'm crazy when she sees me sucking on oxygen during one of my 25(OH)D burn down tests... then says... "You know how to stop them so why do you keep doing this to yourself?"
In reality, the few CH I do have during a 25(OH)D burn down test where I stop just the vitamin D3 until I get the first hit, I catch so early and they're so mild, I usually knock them down by hyperventilating at forced vital capacity tidal volumes with room air for 30 seconds then suck up a lungful of 100% oxygen and hold it for 30 second. Three of these cycles and the CH pain is gone in 3 minutes consuming 12 liters of oxygen.
One of the interesting parts of all this is the time it takes for my CH to recur. My average 25(OH)D serum concentration over the last three years has been around 140 ± 50 ng/mL. If I'm allergy free, it can take almost two months before the CH beast tries to jump ugly. However, if the pollen or leaf mold spore count is excessive and I feel honky (allergic rhinitis), I've had the CH beast trying to jump ugly in as little as three days... That's when a first-generation antihistamine like Benadryl (Diphenhydramine HCL) tablets or Children's Liquid Benadryl come in handy.
The other interesting part of my 25(OH)D burn down tests is the need for magnesium, I learned a long time ago that I can stop taking vitamin D3, but I need to continue taking the magnesium. I start getting hand and leg cramps if I skip the magnesium for more than 3 days.
Take care and good on you... Please keep us posted.
V/R, Batch