All Activity
- Past hour
-
 Arthryon Heat Pain Relief is a topical warming formula designed to provide temporary soothing comfort for muscles and joints while supporting everyday mobility and relaxation. The product is easy to apply and is intended for external use only, making it a convenient option for people who experience occasional muscle tension, stiffness, or minor aches after exercise or daily physical activities. The warming sensation helps create a comforting feeling on the skin, which many users find relaxing after long workdays, strenuous workouts, or repetitive movements. Arthryon Heat Pain Relief is commonly applied to areas such as the back, shoulders, neck, knees, elbows, hands, or legs, depending on the location of minor discomfort. Users should always follow the application instructions provided on the product label and avoid applying the cream to broken, irritated, or sensitive skin. It is also important to wash hands thoroughly after use and avoid contact with the eyes, mouth, and other sensitive areas. While many people appreciate warming topical products for temporary comfort, individual experiences may vary based on factors such as skin sensitivity, activity level, and the nature of the discomfort. Arthryon Heat Pain Relief is not intended to diagnose, treat, cure, or prevent any disease and should not be considered a substitute for professional medical care. Persistent, severe, or unexplained pain should always be evaluated by a qualified healthcare professional. For people with existing medical conditions, allergies, or those who are pregnant or breastfeeding, consulting a healthcare provider before using any new topical product is recommended. Maintaining an active lifestyle, practicing regular stretching, staying hydrated, and following a balanced diet can all contribute to healthy muscles and joints over time. Gentle exercise, proper posture, adequate rest, and stress management may also support overall physical comfort and mobility. Arthryon Heat Pain Relief can be incorporated into a broader self-care routine as a convenient topical option for temporary soothing relief after daily activities or exercise. The non-invasive application makes it simple to use at home, at work, or while traveling, allowing users to target specific areas of occasional discomfort with minimal effort. To achieve the best experience, apply only the recommended amount and use the product according to the manufacturer's directions. If redness, irritation, or discomfort develops, discontinue use and seek medical advice if necessary. Keeping the product out of reach of children and storing it according to the package instructions helps ensure safe use. By combining sensible self-care habits, regular physical activity, and appropriate use of topical products like Arthryon Heat Pain Relief, many individuals can support temporary muscle and joint comfort while maintaining an active and healthy lifestyle. Realistic expectations are important, as results can differ from person to person, and no topical product can guarantee the same outcome for every user. https://arthryon.com/
Arthryon Heat Pain Relief is a topical warming formula designed to provide temporary soothing comfort for muscles and joints while supporting everyday mobility and relaxation. The product is easy to apply and is intended for external use only, making it a convenient option for people who experience occasional muscle tension, stiffness, or minor aches after exercise or daily physical activities. The warming sensation helps create a comforting feeling on the skin, which many users find relaxing after long workdays, strenuous workouts, or repetitive movements. Arthryon Heat Pain Relief is commonly applied to areas such as the back, shoulders, neck, knees, elbows, hands, or legs, depending on the location of minor discomfort. Users should always follow the application instructions provided on the product label and avoid applying the cream to broken, irritated, or sensitive skin. It is also important to wash hands thoroughly after use and avoid contact with the eyes, mouth, and other sensitive areas. While many people appreciate warming topical products for temporary comfort, individual experiences may vary based on factors such as skin sensitivity, activity level, and the nature of the discomfort. Arthryon Heat Pain Relief is not intended to diagnose, treat, cure, or prevent any disease and should not be considered a substitute for professional medical care. Persistent, severe, or unexplained pain should always be evaluated by a qualified healthcare professional. For people with existing medical conditions, allergies, or those who are pregnant or breastfeeding, consulting a healthcare provider before using any new topical product is recommended. Maintaining an active lifestyle, practicing regular stretching, staying hydrated, and following a balanced diet can all contribute to healthy muscles and joints over time. Gentle exercise, proper posture, adequate rest, and stress management may also support overall physical comfort and mobility. Arthryon Heat Pain Relief can be incorporated into a broader self-care routine as a convenient topical option for temporary soothing relief after daily activities or exercise. The non-invasive application makes it simple to use at home, at work, or while traveling, allowing users to target specific areas of occasional discomfort with minimal effort. To achieve the best experience, apply only the recommended amount and use the product according to the manufacturer's directions. If redness, irritation, or discomfort develops, discontinue use and seek medical advice if necessary. Keeping the product out of reach of children and storing it according to the package instructions helps ensure safe use. By combining sensible self-care habits, regular physical activity, and appropriate use of topical products like Arthryon Heat Pain Relief, many individuals can support temporary muscle and joint comfort while maintaining an active and healthy lifestyle. Realistic expectations are important, as results can differ from person to person, and no topical product can guarantee the same outcome for every user. https://arthryon.com/ -
Averos Patches sind speziell entwickelte Pflaster zur Unterstützung der männlichen Vitalität und des allgemeinen Wohlbefindens. Sie bieten eine praktische und unkomplizierte Möglichkeit, die tägliche Pflegeroutine zu ergänzen, ohne dass Kapseln oder Pulver eingenommen werden müssen. Dank ihres benutzerfreundlichen Designs lassen sich die Pflaster einfach auf die saubere und trockene Haut aufbringen und bequem über mehrere Stunden tragen. Viele Männer entscheiden sich für Averos Patches, weil sie nach einer komfortablen Lösung suchen, die sich problemlos in den Alltag integrieren lässt. Die regelmäßige Anwendung kann dabei helfen, das persönliche Wohlbefinden zu unterstützen und einen aktiven Lebensstil zu begleiten. Besonders Männer mit einem anspruchsvollen Berufs- oder Familienalltag schätzen Produkte, die einfach anzuwenden sind und keine aufwendige Vorbereitung erfordern. Averos Patches werden häufig im Zusammenhang mit Themen wie männlicher Energie, Vitalität und Selbstvertrauen erwähnt. Ein gesteigertes Wohlbefinden kann dazu beitragen, sich körperlich und mental ausgeglichener zu fühlen und den Alltag mit mehr Motivation zu bewältigen. Für optimale Ergebnisse empfiehlt es sich, die Anwendung gemäß den Herstellerhinweisen durchzuführen und die Pflaster regelmäßig zu verwenden. Gleichzeitig sollte berücksichtigt werden, dass Nahrungsergänzungs- und Wellnessprodukte eine ausgewogene Ernährung, ausreichend Bewegung und einen gesunden Lebensstil nicht ersetzen können. Eine abwechslungsreiche Ernährung, ausreichend Schlaf und regelmäßige körperliche Aktivität bilden weiterhin die Grundlage für langfristige Gesundheit und Leistungsfähigkeit. Wer seine allgemeine Fitness verbessert, kann häufig auch sein persönliches Wohlbefinden positiv beeinflussen. Averos Patches sind für Männer gedacht, die ihre tägliche Wellness-Routine sinnvoll ergänzen möchten und Wert auf eine einfache Anwendung legen. Da jeder Körper unterschiedlich reagiert, können individuelle Erfahrungen mit dem Produkt variieren. Es ist daher sinnvoll, realistische Erwartungen zu haben und bei bestehenden gesundheitlichen Beschwerden oder der Einnahme von Medikamenten vor der Anwendung ärztlichen Rat einzuholen. Die Pflaster sind keine Arzneimittel und dienen nicht der Diagnose, Behandlung, Heilung oder Vorbeugung von Krankheiten. Aussagen über eine Verbesserung der sexuellen Leistungsfähigkeit oder eine Behandlung von Erektionsstörungen sind wissenschaftlich nicht ausreichend belegt und sollten nicht erwartet werden. Stattdessen können Averos Patches als Bestandteil einer gesundheitsbewussten Lebensweise betrachtet werden, bei der Selbstfürsorge, Bewegung und eine ausgewogene Ernährung im Mittelpunkt stehen. Wer auf Qualität, Komfort und eine einfache Anwendung Wert legt, findet in Averos Patches eine praktische Ergänzung für den Alltag. Durch die Kombination aus konsequenter Anwendung, gesunden Gewohnheiten und einem aktiven Lebensstil können Männer ihr allgemeines Wohlbefinden unterstützen und ihre persönliche Vitalität langfristig fördern. https://averospatches.de/
-
andaverospatches joined the community
- Today
-
 88aavnappp changed their profile photo
88aavnappp changed their profile photo -
88aavnappp joined the community
-
 Ao88network joined the community
Ao88network joined the community -
 uy88gg joined the community
uy88gg joined the community -
 loansiteclickn joined the community
loansiteclickn joined the community -
 thereelgme joined the community
thereelgme joined the community -
 danielkang joined the community
danielkang joined the community -
 bags168com11 joined the community
bags168com11 joined the community -
 viskaencan joined the community
viskaencan joined the community - Yesterday
-
 ad88innet changed their profile photo
ad88innet changed their profile photo - Last week
-
 Geronimo changed their profile photo
Geronimo changed their profile photo -
Mille mercis pour ton message de soutien
-
 Uy8888org changed their profile photo
Uy8888org changed their profile photo -
 go88zacom2 changed their profile photo
go88zacom2 changed their profile photo -
 shbet800com01 changed their profile photo
shbet800com01 changed their profile photo -
CH past two mornings after lowering Verapamil but still very mild.
-
-
 gamebaidoithuonggcom changed their profile photo
gamebaidoithuonggcom changed their profile photo - Earlier
-
This is especially anecdotal, but in addition to my longtime baseline tinnitus, 1.5 years ago or so I started getting some WTF!!?? crazy, crippling, deafening loud blasts in one ear that would last up to 24 hrs before receding. The ear doc recommended steroid shots in the middle ear. I did the series of 3. It seemed to help some. Years ago I had read that about the only supplement that could 'maybe' help with tinnitus was Astaxanthin. So I got some and took it religiously, but that brand became unavailable, so I switched to another. Then 6 mos ago I went off the new brand to see if it was causing a rash. It wasn't, BUT at that point my loud blast episodes completely ceased and haven't returned since. Could be coincidental, but I strongly suspect the new brand of astaxanthin could have been backfiring on me! It was cheaper than others - hmmmm.
-
I can see why you would be apprehensive about the Lenire thing, since "a small mouthpiece delivers mild electrical pulses to the tongue, activating the trigeminal nerve to enhance neuroplastic changes in the brain." Gotta say, that does sound like a risk. I remember when I first developed tinnitus. I've had a lot of very bad, chronic pain in my life, but I was sure I was going to go crazy and/or kill myself from the tinnitus. Maybe you'd had it a long time and haven't figured out a way to cope. For me, it has almost completely faded into the background. This was true for my brother, too, who as a professional musician was deeply bothered by it. Last time I asked him how his tinnitus was, he said, "I don't really think about it unless some asshole asks me how I'm doing." Haven't asked him again. Noticing mine more right now, of course, but I know it's going to fade back into the background.
-
After I noticed I had tinnitus, I just started with noise, more specific, rain, storms, water noises when trying to fall asleep. It made me used tonit again (because I’ve had it as long as I remember, I’ve only ever known the ringing ‘sound of silence’) just try to get used to it, I honestly laugh at myself when I recall that period, I didn’t have CH yet. I know what it is and it is not easy, I know, but today I’d wish I only had tinnitus. try apps like resound tinnitus relief, it helps.
-
I wanted to see if anyone has used the Lenire treatment for Tinnitus and whether or not there you experienced any negative effects with regards to your cluster headaches
-
 phimhayokco2 changed their profile photo
phimhayokco2 changed their profile photo -
 kyloveky1 changed their profile photo
kyloveky1 changed their profile photo -
Thanks! I've increased the dosage of KLOW slightly to what I'm seeing others doing so I'm now getting per day: 2.5mg GHK-CU 500mcg BPC 157 500mcg TB-500 500mcg KPV Forgot to update yesterday but it was CH free, and that was just 3 days after lowering Verapamil. I did not lower it yesterday just to see if it was a fluke but there was again no CH this morning, so I will lower it today. I've had this other type of pain in the trigeminal area (temple, cheek, above/behind the eye, sometimes back to the neck) in between CH for years. Same side as the CH, completely unilateral. It used to come in months long episodes (3-4) and then it was gone for a couple of months until returning again. Last 2 years its been constant, sometimes I get 20-30 minutes at waking up until it starts. It's like the whole left side of my head/brain is inflamed, and there is a burning sensation and some pain in the trigeminal area constantly. With that I get intermittent stabbing pain, so its like a sawtooth pattern where I'm constantly on 3-4 in pain and then there is second long stabs that brings pain up to 7-8. When its really bad the stabs can come like every 10 seconds and go on for hours. Sleep sort of "resets" everything, but then the pain comes crawling back fairly quickly. I have tried Indomethacin against this with some success, some of the stabbing stopped but after I had another bout of CH it feels like its almost back to where it was before I started taking it. Felt a lot of improvement from KLOW on this pain in the first couple of days but effect seem to be wearing off. Gabapentin has also worked for this sort of pain, but only for 3-5 days before I've needed to increase dosage, until side effects become intolerable. I'm convinced its neurological, my neurologist first claimed it was muscular but I've been to literally hundreds of chiropractors and other sort of mechanical practitioners (neck, shoulders, jaw, teeth etc etc) without result. I think I've tried all of the medications you could think of except Pregabalin. I've also tried hundreds of supplements and things like progesterone, methylene blue, cyproheptadine, aspirin etc, and nothing seem to work.
-
I'm really interested in this approach and your findings. Please keep updating us like you're doing. Every bit of knowledge helps!
-
 luck8day1 changed their profile photo
luck8day1 changed their profile photo -
CH again at 6, a bit more pain this time but nothing like a full blown attack, lasted maybe 2 minutes. The lingering pain does seem to be improved still.
-
Was woken up by CH again at 6AM but the pain lasted for less than a minute and was very mild compared to a regular attack, no oxygen needed since I started taking KLOW. I am now on 1+1+2 of 80mg Verapamil and will continue to decrease when I reach a CH free day. I am fairly confident its the lowering of dosage triggering the CH. I "shouldn't" be having CH at all this year, I've been having episodes every two years since 2019 but had a couple of weeks in May this year that was very stressful and caused the CH to flare up.
-
No problem! Yes, I am not vouching for this either, I should have said this right away: There is zero research / safety profile for these peptides in humans, this is highly experimental. I did however wake up without CH this morning, but impossible to say if its the KLOW, it really shouldn't be after 2 injections. I'm on day 6 of lowering verapamil, so it could just be that I stabilized here on the new dosage. Will drop another tablet today and see what happens.
-
Thank you for this!!!! Not vouching for or saying anything against it. Looking forward to reports. This page seems like a pretty good discussion: KLOW — research profile · Peptide Research
-
Anyone tried some of the peptides that's becoming popular now? I started KLOW yesterday, which is a blend of peptides that targets multiple pathways involved in healing, inflammation control, and cellular repair. I've only taken one dose, but this mornings attack did seem dampened roughly 50% compared to prior days. I also feel a lot better after the attack, my day is usually ruined by lingering pain, but now its very manageable. Remains to see if this is one of those things that works great for a short time to never work again later, or if it gives some longer lasting effect. Will report back.
-
when I finally stopped taking verap i dropped it off from 120 to 0. I did and still do have oxygen, 5hr drinks and a few other tricks I use to abort when needed. I do not get any more or less clusters but I did get rid of most of the side effects. I was up around 1020 a day and that sucked. If I were to go back in time I would not have started taking it at all.
-
I am trying to taper down but as soon as I drop even 1 tablet (I'm on 2x80mg three times per day) I start waking up at 6AM because of CH. I have tapered down before, and it was a pain in the a**, because just like now it seems to aggravate the CH with each lowering of dosage. I am wondering if I should just drop it to zero right away and push through the headaches that will undoubtedly come, I have oxygen at home. Anyone ever tried that?
-
Nice, I hope this keeps working for you
-
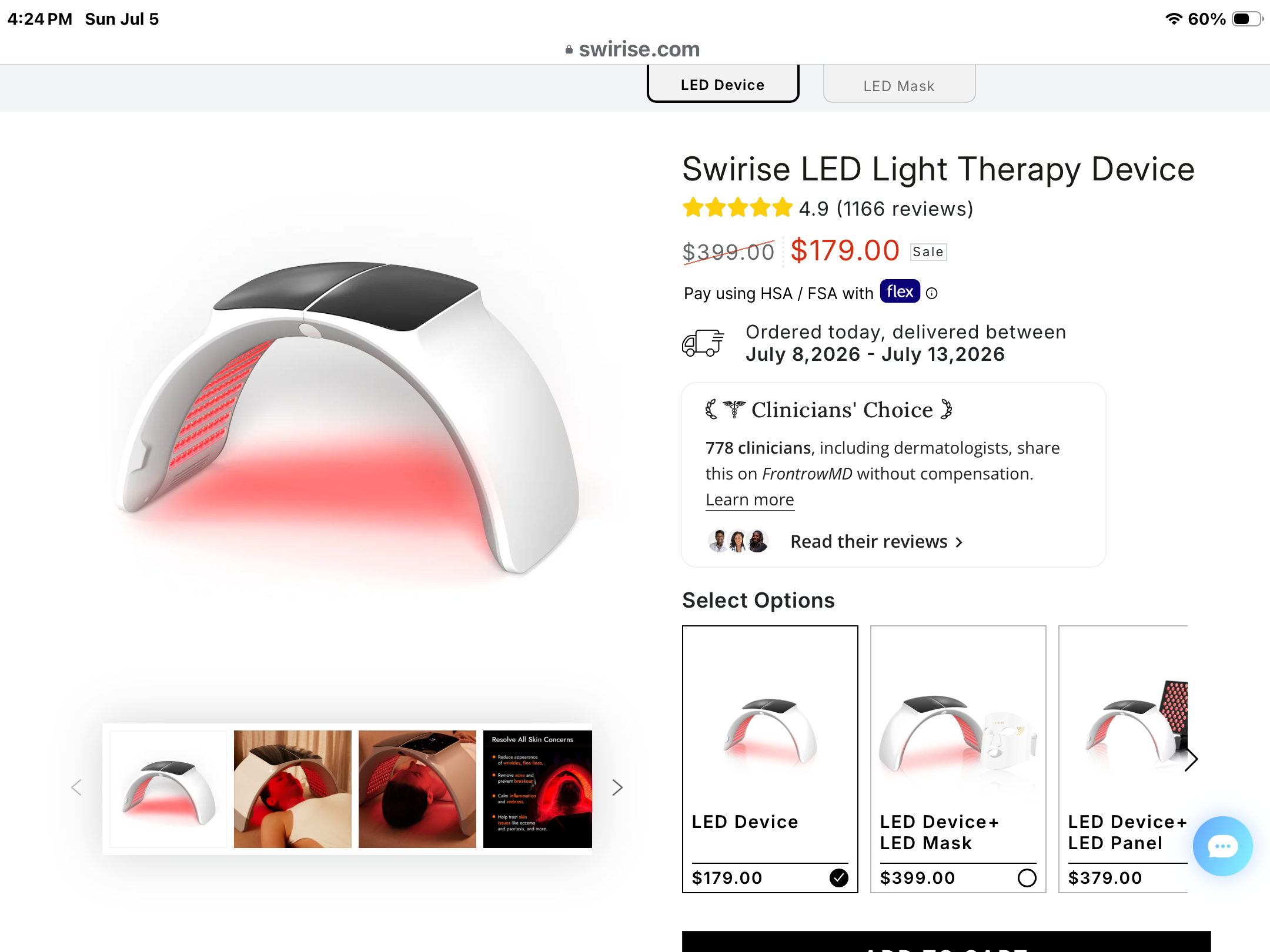
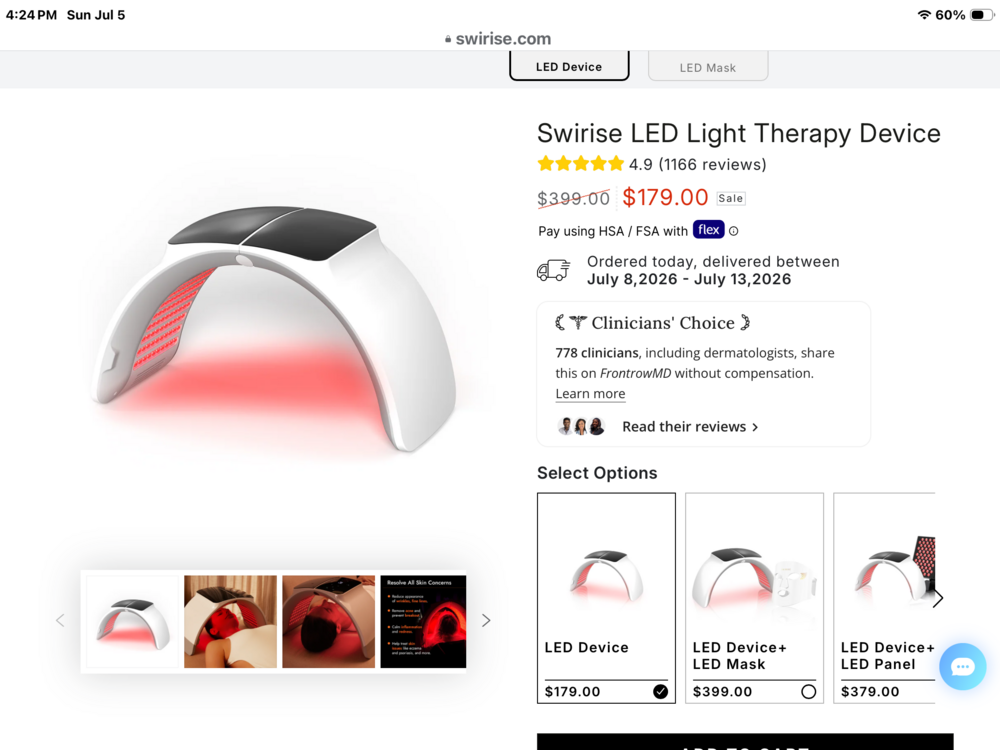
Hey guys, I purchased this device and have been using it for 40 minutes a day when I wake up. I lay on my back eyes closed in a dark room for the 40 minutes using the green light mode. I have been Migraine free since I have started using it. Its been a few weeks now without a migraine which for me is amazing. I have been having migraines 3 to 5 days a week for 40 plus years.
-
I get that way from time to time. Good fishing in Wi
- 1 reply
-
- 2
-

-
Thanks to all that responded to my post in Theory and Implementation, some how deleted the post when responding. Think my head isn’t firing on all cylinders. I will continue to read and follow along for now. Foggy head and tired Cheesehead in Wisconsin :|
- 1 reply
-
- 2
-
-
Its 6am, just about to make coffee - reading this, man - awesome awesome awesome and may your remission continue long into the future. There is nothing better than reading of a fellow warrior getting pain free. Made my day. Cheers brother Jimmy! Craig.
-
@FunTimes very helpful to know this. Thank you!
-
DMT use in Cluster Headache: Interim Analysis of an International Survey (S23.003) | Neurology "Among those who used DMT to abort attacks (n = 85), the majority reported it completely eliminates pain (67.5%) and that it works every (45.7%) or almost every (35.8%) single time. Over half reported that DMT worked in under 30 seconds, and all participants reported either no change or an improvement in their health with DMT use."
-
- 2
-


.thumb.jpg.24dde7ef3152d6d31b9546e3fec3b26d.jpg)
.thumb.png.d237bb0dbb7bd8ac08da8f08a1ba65f8.png)