Article Sections
Cluster Headache is a primary neurovascular headache classified by the International Headache Society (IHS) diagnostic criteria and grouped with similar conditions known as the Trigeminal Autonomic Cephalalgias8. Cluster headaches are characterized by strictly one-sided attacks that come on quickly, reaching their peak in just a few minutes. They can last 15-180 minutes or longer and re-occur up to eight or more times each day4. The pain is often described as an icepick, hot dagger, pronged side of the hammer that is unrelenting throughout the attack. Others liken it to a brain freeze, lasting up to three hours instead of a few seconds.
These attacks cause patients to exhibit agitation and restlessness such as pacing and hitting themselves. Cluster headaches are typically localized around the eye and temple4 and come with several one-sided autonomic symptoms—swollen or droopy eyelid, teary or red eye, forehead or facial sweating, runny or stuffy nose, contracted pupil2. While cluster headaches only affect one side of the head, they can switch sides.
What Causes Cluster Headaches?
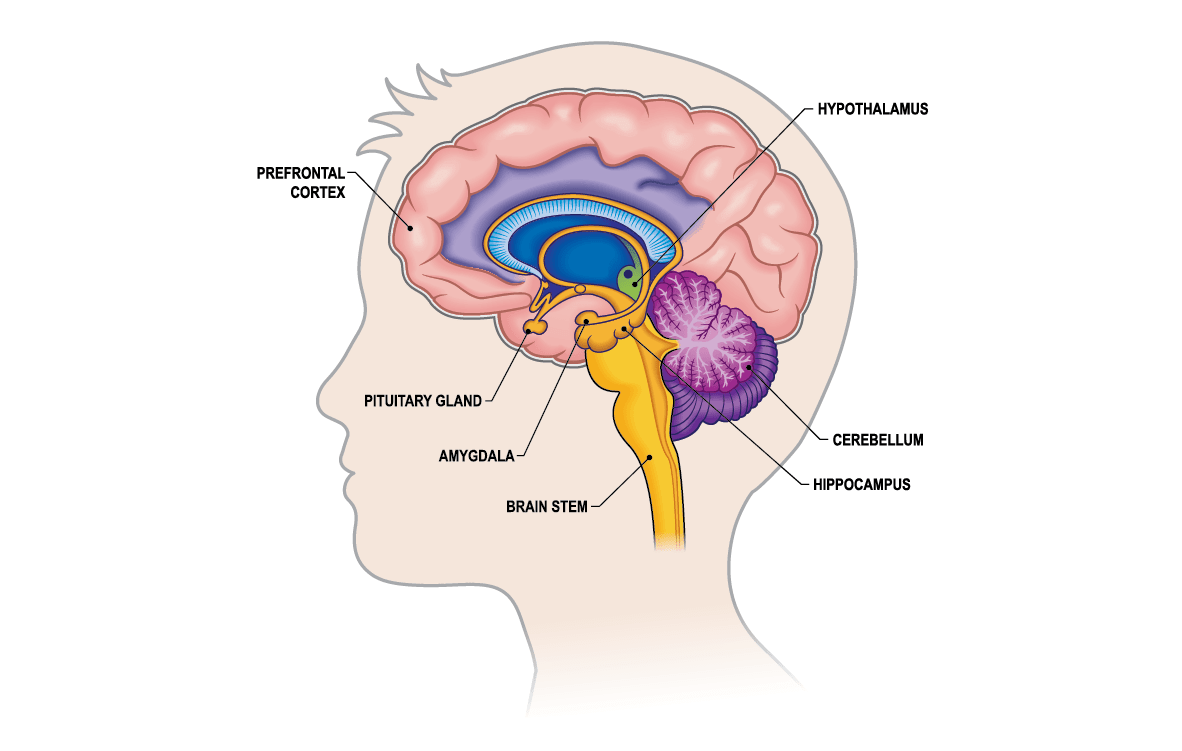
This neurological condition has no known cause, but there is a plausible theory that it’s due to a dysfunction in the hypothalamus, specifically the posterior hypothalamus2. The hypothalamus has many jobs including maintaining quality of sleep, times of the day, changing seasons. With the help of the pituitary glands, it moderates hormone production such as testosterone, estrogen, melatonin and serotonin5. Since REM (dream) sleep is a common trigger for cluster headaches, it makes sense that hypothalamic dysfunction could be to blame, but there are other players on the field, including the sphenopalatine ganglion and the trigeminal nerve, which can swell up to seven times it’s natural size during an attack3. A 2019 medical review reported a periodic dysfunction of the hypothalamus in cluster headache patients as well1.
Cluster headaches impact approximately .1% of the population, similar to the number of people afflicted with multiple sclerosis and Autism spectrum disorder. The high frequency and intensity of the attacks dramatically decreases quality of life and often leads to suicidal ideations, as this condition is nicknamed “Suicide Headaches”4.
Diagnostic criteria — Episodic Vs. Chronic
Approximately 85-90% of people with cluster headaches are episodic with the remaining experiencing the chronic form of the disease. Some “clusterheads” switch from episodic to chronic and vice versa. The International Headache Society (IHS) released the latest cluster headache diagnostic criteria in 2016, but much of it stayed the same from the previous 2010 guidelines. It includes4:
- Episodic Cluster Headaches Must experience bouts of attacks lasting seven days to one year which are then separated by a period of remission lasting at least one month.
- Chronic Cluster Headache: Experiences attacks on a daily basis for more than one year followed by a remission which lasts less than one month or with no remission at all.
Whether you’re episodic or chronic, you must also meet these criteria according to the International Headache Society classifications:
- Severe, unilateral orbital, supraorbital, temporal pain lasting 15 minutes to three hours.
- Frequency is one every other day or eight or more each day.
- Each attack comes with at least one of these autonomic features, which occur on just one side of the head or face—the same side as the pain:
- Nasal congestion
- Rhinorrhea (runny nose)
- Forehead or facial sweating
- Miosis (Constricted pupil)
- Conjunctival injection (tearing or red eye)
- Eyelid oedema (swollen, drooping eyelid)
- Restlessness or agitative behaviors
There’s also the term “Probable Cluster Headache” for those who meet all but one criterion of the IHS guidelines.
Despite the severe nature of cluster headaches and the depression, isolation, and suicidal thoughts that accompany the attacks, it takes an average 5.3-6.6 years for a patient to be accurately diagnosed, and this number is often higher for women who are typically misdiagnosed with migraine disease for years9. Cluster Headache was considered a middle-aged man’s disease for decades so the previously published ratio of 8:1 or 6:1 is actually down to 2:1 or 3:1 now that women are treated correctly4.
Both sexes can develop cluster headaches at any age, but there seems to be an increased rate of men having their first attack in their early teens or around age 30. Similarly, women seem more likely to develop cluster headaches in their late teens or early twenties and then again around the age of 50. This could have something to do with the hormones involved in the hypothalamus as these are the times in your life that you experience extreme hormonal changes4. It’s also important to mention that each patient needs an MRI to rule out other brain disorders6.
Treatments for Cluster Headaches
The first thing a physician must do after diagnosing a patient with cluster headaches is write a prescription for high-flow oxygen through a nonrebreather mask at 12-15 liters per minute7. The second step should be a referral to a headache specialist or neurologist6. There are several options for medications, devices and alternative treatments to combat the cluster headache “beast.” Psilocybin mushrooms and LSD have been and continue to be studied as effective treatments for cluster headaches too.
- High-Flow Oxygen
- Abortive Treatments
- Preventive Treatments
- Alternative Treatments (including psilocybin, LSD, ketamine, and LSA seeds)
According to guidelines published by the American Headache Society, these abortive medications are recommended using a scale of efficacy8:
Level A Advice for Aborting Cluster Headaches: Established as effective
- Sumatriptan Subcutaneous Injection 6mg
- Zolmitriptan Nasal Spray 20mg
- High-flow oxygen at 15lpm or higher
Level B Advice for Aborting Cluster Headaches: Probably effective
- Sumatriptan Nasal Spray 20mg
- Zolmitriptan Oral 5mg and 10mg
- Sphenopalatine Ganglion (SPG) Stimulation
Level C Advice and Level U Advice for Aborting Cluster Headaches: Possibly effective or insufficient evidence
- Cocaine/Lidocaine 10% Nasal Spray (C)
- Octreotide Subcutaneous 10ug (C)
- Dihydroergotamine Nasal Spray 1mg (U)
- Somatostatin 25 ug (U)
- Prednisone 30mg (U)
“The oral route of administration should generally be avoided since the pain-relieving effect is delayed compared with that of the subcutaneous or intranasal routes of administration,” wrote Dr. Jan Hoffman.
The AHS also have guidelines for prophylactic (or preventive) treatment of cluster headaches which includes:
- Level A: Suboccipital Steroid Injection, a single injection or a series of injections.
- Level B: Civamide Nasal Spray, 100 ul of 0.025% civamide.
- Level C: Lithium 900mg daily, Verapamil 360mg daily, Warfarin with a goal ratio of 1.5-1.9, or Melatonin 10mg daily.
- Level U: Frovatriptan 5mg daily, Capsaicin intranasal used in a cream twice daily, nitrate tolerance, or prednisone 20mg every other day.
It’s recommended to start with the Level A advice and if those options fail to provide relief, you can try Level B, C, and ultimately U if the benefits outweigh the risks. There are also newer options that may help you get relief such as the gammaCore® Vagus Nerve Stimulator for episodic cluster headaches, and Emgality® the first-ever FDA-approved drug for episodic cluster headaches.
References:
- Burish, M. J., Chen, Z., & Yoo, S.-H. (2018). Emerging relevance of circadian rhythms in headaches and neuropathic pain. Acta Physiologica, 225(1). doi: 10.1111/apha.13161
- Goadsby, P. Cluster Headache – Update on a Common Neurological Problem. Practical Neurology 1. 2001; (1): 42-9.
- Gray, H. (2000). IX. Neurology. 5e. The Trigeminal Nerve. Gray, Henry. 1918. Anatomy of the Human Body. Retrieved March 24, 2015, from http://www.bartleby.com/107/200.html
- Hoffmann, et al. Diagnosis, pathophysiology, and management of cluster headache. The Lancet Neurology. 2017; Series 1.
- Konakchieva, R., Mitev, Y., Almeida, O.F. and Patchev, V.K. (1997), Chronic melatonin treatment and the hypothalamo-pituitary-adrenal axis in the rat: Attenuation of the secretory response to stress and effects on hypothalamic neuropeptide content and release. Biology of the Cell, 89: 587-596. doi: 10.1111/j.1768-322X.1997.tb01036.x
- Lane, M.D., J.(2015, February 10). Cluster Headaches [Personal interview].
- McGeeney, B. (Speaker) (2014, September 19). Exploring Cluster Headache. 9th Annual Clusterbusters Cluster Headache Conference. Lecture conducted from Clusterbusters, Nashville.
- Robbins, et al. Treatment of Cluster Headache: The American Headache Society Evidence-Based Guidelines. Headache: The Journal of Head and Face Pain. 2016; 56(7), 1093-1006.
- Rozen, et al. Cluster Headache in the United States of America: Demographics, Clinical Characteristics, Triggers, Suicidality, and Personal Burden*. Headache: The Journal of Head and Face Pain. 2011: 52(1), 99-113.