Leaderboard




Popular Content
Showing content with the highest reputation on 08/18/2021 in Posts
-
Hey DD, AlanK, All, The 80 ng/mL "sweet spot" (target 25(OH)D3 serum concentration) is actually the mean 25(OH)D3 serum concentration reported by 80% of participants in the online survey who experienced a favorable response to this treatment protocol. If you look at the following normal distribution chart of CHer reported lab results for 25(OH)D3 after ≥ 30 days on this treatment protocol below, half of these CHers required a higher 25(OH)D3 serum concentration up to 180 ng/mL to achieve a CH pain free response. What this really means is they needed a larger vitamin D3 loading dose/longer loading schedule and higher vitamin D3 maintenance dose than 10,000 IU/day. I've spent a good deal of time working with the CHers (and their doctors) who didn't respond to this treatment protocol using a 25(OH)D3 serum concentration target of 80 to 100 ng/mL. What they had in common was their serum PTH was still in the mid-Normal range. When they increased their vitamin D3 intake with loading doses between 100,000 IU/day and 150,000 IU/day, their PTH dropped to a low-Normal range and they started responding with a significant reduction in CH frequency or they experienced a CH pain free response. What's also significant is their serum calcium concentration remained within its normal reference range. This vitamin D3 treatment protocol has evolved slightly over its 10 years existence. When we shifted the type of vitamin D3 from the oil-based liquid softgel formulations to the Bio-Tech D3-50 50,000 IU water soluble form of vitamin D3 in mid 2018, we saw an increase in the 30 day significant response rate from 80% to nearly 90% and an increase in the 30 day CH pain free response rate from 54% to 60%. Shifting from the generic vitamin B 50/100 complex to the Methyl Folate + B complex also helped. It's important to note these changes were not made in a vacuum. This is a patient-centered and patient developed treatment protocol so "we" made these changes after observing the increase in efficacy. The "We" is critical here as these changes/improvements could not have been made without input, feedback and active participation by the CHers and their PCP or neurologists following this treatment protocol. Accordingly, in a very real sense, this is Your treatment protocol. It's also important to note that I have also actively participated in these changes to the treatment protocol taking larger vitamin D3 loading doses elevating my serum 25(OH)D3 higher and taken higher vitamin D3 maintenance doses to maintain that higher 25(OH)D3 serum concentration. Over the last four months, several of us have taken a loading dose combination of two (2) Bio-Tech D3-50 capsules and 0.5 mL of the Micro D3 nanoemulsion taken sublingual, for a total daily loading dose of 140,000 IU of vitamin D3. This combination resulted in a rapid and effective elevation of the 25(OH)D3 serum concentration and more importantly, a cessation of CH without going bust on serum calcium or PTH. The following 4-Year chart of my labs for serum 25(OH)D3, calcium and PTH tells the story. My PCP had no problem with my 25(OH)D3 serum concentration at 277 ng/mL as my serum calcium remained within its normal reference range and my PTH serum concentration didn't get too low. He did order a 24 Hr urine collection to make sure I wasn't dumping calcium in urine. Here are the results: Tests: (1) Calcium, 24Hr, Ur w/Creatinine (003324) 28 May, 2021 Calcium, Urine 24hr 146 mg/24 hr 26-354 Calcium/Creat. Ratio 118 mg/g creat. 14-318 Serum 25(OH)D3 at 277 ng/mL (692 nmol/L). No Hypercalcemia and No Hypercalciuria At this point I need to make the following disclaimer. The vitamin D3 treatment protocol discussed above is solely for educational purposes regarding potentially beneficial therapies for Cluster and Migraine Headache. Never disregard professional medical advice because of something you have read on our website and releases. It is not intended to be a substitute for professional medical advice, diagnosis, or treatment in regards to any patient. Treatment for an individual patient should rely on the judgement of your physician or other qualified health provider. Always seek their advice with any questions you may have regarding your health or medical condition. Take care and please keep us posted, V/R, Batch1 point
-
Batch, Been having some success. Strangely, my clusters this cycle have turned into mostly migraines. More manageable, but it's not something I'm used to. Is this common? Felt like I was making progress and dropped the D3 yesterday to 50k only to get hit this AM. If you have any insight here, let me know. My plan is to continue with the 100k/day for up to a week if needed and then taper down to 50k/day for a week and then onto maintenance dose. My labs are scheduled for the end of this month. Also, the double magnesium does a number on my stomach. I've found splitting the pills up and taking after the two biggest meals of the day helps a lot. If anything I've found myself eating more before taking the pills to offset the GI issues.
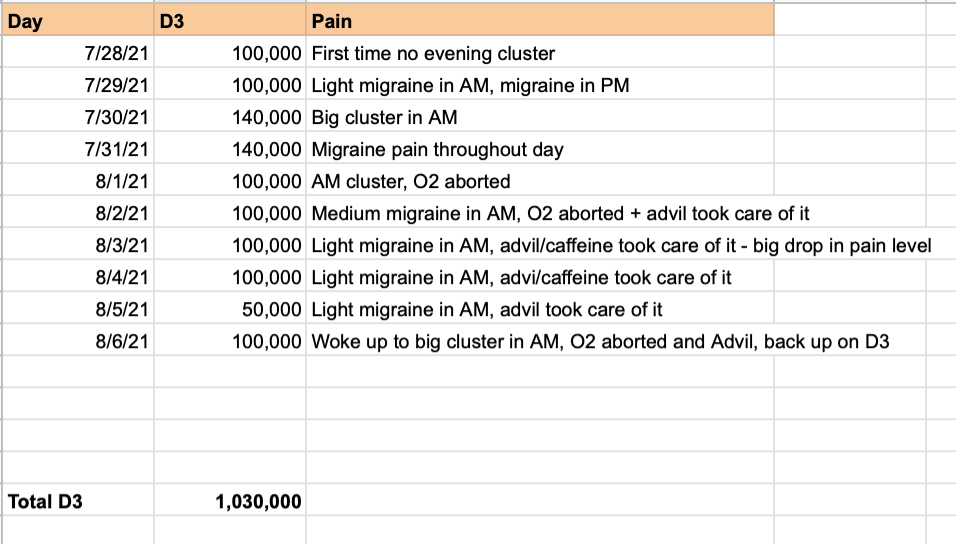 1 point
1 point