Cast Iron
-
Posts
61 -
Joined
-
Last visited
-
Days Won
1
Everything posted by Cast Iron
-
I can not answer your questions, but can give you my story which is quite similar. Started as episodic with 240 verap a day. The physical impact is something I noted right away, less stamina, tired, but accepted it. After a while when I was off-cycle I tried to lower the verap, but after a week or so, the hits returned and into a new cycle. This made me causious to try this again. After a year or so I gave it another try, but again the same pattern. But this time going back to the previous dose did not help, I had to up the dose with another 120mg. Eventually my intake of verap became high, 840mg, and I did not want to up this to 960, so the doc gave me two additional medicines, sandomigran and naratriptan. This stabilized the cycle in 2018 with a few hits a day, but in hindsight, this was the moment I got chronic. I use the slow release and what people tell that it stacks in your body is true, but also in my case this is intended. I need to build a medicine barrier quite high to hold the beast at bay, because I have a big and vicious beastie. 2019 I was in the trail group for Aimovig and to qualify had to lowered my verap from 840 to 480. After a week, the hits went from 7 to 10 a day. Not good. Again exactly the same pattern that I had seen before, apparently one can get accustomed to the intake of a medicine quite rapidly. Aimovig did not work out, but the good thing was that my new intake was only 720mg. Last year started the D3 and after a few months decided to lower the verap to 600mg. Definitely not a good idea because I am now in cycle for 14 months on 720mg + the addition meds. My take on this, maybe you can try 240mg slow release to build a barrier during the day, or when you lower to 120mg also consider the slow release with a prednisone tapper. Lowering verap did not work for me, but truly hope it can make a hugh difference for you.
-
Various Questions About Spikes/Picks to the Brain ETC..
Cast Iron replied to BoscoPiko's topic in General Board
I regularly have spikes on my left temple, while my CH is on my right. These spikes are in many cases the onset of an attack, but not always. It makes me aware that the beast is awake and wants to come out to play. This does not mean I stop doing what I was doing of want to do, except when I kinda feel an attack is eminent, I start the O2. What also helps me when I have a little spike is to go outside for a walk in the fresh air, this also clears the spike quite rapidly. Some people have spikes in the Great Occipital Nerve which is often an indication that they will soon enter into their cycle. I see the spikes on my temple normally only when in cycle, but on the other hand I am chronic. Over time I can now feel what kind of spike it is, is it a random one, or because I have eaten something that is on the ‘NOGOOD’-list or went to bed far too late. As J says, the beast comes in different forms and shapes, where a spike for one is the start of a cycle, where for others it is a morphing of a regular pattern to the next. ATB -
I feel very sorry that you had to go through that. Nothing as bad than to see your loved ones go through so much pain and nothing you can do at that moment, and have to wait your turn in the ER. I think we all can relate to your situation. What I would like to suggest is that you need to have prescriptions for the rescue meds. First you need to have Oxygen as a first abortive, its safe, cheap and portable to wherever you go. Using this on the onset of an attack with a flowrate of 25L/m has a high efficacy of breaking the attack. Second, if O2 is not helping to abort, you need to have Sumatriptan injections as your rescue to prevent having to go to the ER. Sumatriptan is a big hammer that will abort and make the pain go away within 5 minutes. You’ll want both of them to make sure you are not dependent on the ER. On very severe attacks, both sumatriptan and O2 can be combined. All the best Alex
-
@trjonas In the last years I have tried to lower my verapamil and every time I ended up in really bad cycles. It's like my system really needs a certain level of verapamil to keep it at bay. You can also say that I have built a dependency on 720mg (I was on 840 in one bad cycle), and I won't deny that. So I took the plunge into the D3 to hopefully break the dependency and cause I had read so many success stories about it. But like you say, for some it works for others not. Upping my intake to levels above 300...well I have to read up about it because I do not know what the (side)effects might be. But if this works for you, then I could not be happier for you. Cutting a third on your meds does probably mean you'll have a significant part of your normal life back. All the best Alex
-
Hello Trjonas, No worries, but yes I have a big beast to deal with, constantly and never ending story. As a chronic I try to keep it caged with all the medicines, D3, changes to my daily habits and foods, but it's strong and comes out to 'play' very often. Have to say though that i am getting very tired, but can't let it win. Optimism is a virtue. As for my lab results, the first one is the the baseline, on the second Batch gave his 'blessing' that the numbers were at par: -D3: 64 - 211 -B12: 88 - 128 -PTH: 2,2 - n/a -Calcium: 2,47 - 2,26 -Eosinophil: 0,1 - 0,1 -CRP: 8 - 6 All the best Alex
-
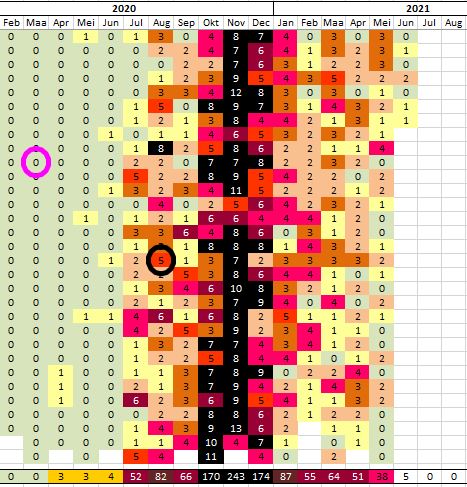
For every success story there is a counter balance, like mine. After consulting Batch I started the D3 last year March as I was looking for a solution to decrease my intake of verapamil before my next cycle would start. After 1,5 month my blood serums were at par and removed one 120mg verapamil to 600mg daily dose (plus naratriptan, sandomigran), hoping the D3 would keep the beast at bay. What happened was not what I expected, my cycle started and ramped up to sometimes 12 attacks a day. Did the Emgality, GON injection, prednisone but all to no avail. On a certain month I had >240 attacks (pic below). Also my normal cycle was extended from 5 months to a full year now and in between I had to up my verapamil to 720 again. Still I am in the aftermath of my cycle, and actually scared this will roll over into a new one which normally happens around May/June. Alex
-
Pebbles, got my Pfizer shot last wednesday with no effect on my cycle.
-
Hello Mr Watts, So good that you have found this forum, too bad that you’re now part of the family. I live in the Netherlands too and there are a couple of things you can consider already. Get a prescription for verapamil as a preventive as long as you do not have O2. O2 is the safest and quickest abortive, but also get some Sumatriptan as an abortive if O2 is not working anymore or the attack is just too severe. If I were you I would change to another neurologist. Mine is Dr. Couturier of the Boerhaave Clinic in Amsterdam who is an expert in this field of CH in the Netherlands. He has helped me tremendously and will prescribe O2 immediately as well as the meds you are going to need. All the best!
-
Pebbles, as a CCH lets see as I am up for the first shot of Pfizer or Moderna next week
-
In high cycle I've been using up to 6 a day where i was having 12-14 attacks a day and O2 was just not sufficient to abort. Under 'normal' circumstances O2 should be the preferred option, but in my high cycles the attacks are just too severe and extremely painful. Yes it is absolutely not recommended to take so many a day but it was the only option to get the beast at bay for a couple of hours. Now i am in my lower cycle and use 1 a day (for 5 months already), the others I can manage with O2. As to what @CHfathers recommends to split, nowadays there is also the 3mg available instead of the 6mg, which work also for me in low cycle although they work not as quick as the 6mg. On the other hand with the 3mg there are less rebounds. All the best
-
Your take on daytime sleeping / Napping - is it really that bad
Cast Iron replied to Archimedes's topic in General Board
Of all people we are the ‘different’ ones in many aspects. Drinking energy shots before sleeping or during the night to abort an attack ànd go back to sleep is not what many people can do or would advise. The reverse is also true, at least in my case, I can not have a daytime nap because it will definitely trigger the beast to wake up and have some fun. Yes, this really forces me to do something else and wait for the normal sleep cycle to begin. It’s what my sleep neuro advised me to do, as well as trying to avoid bright lights (especially with a lot of blue in it) during the day and night in case I am pacing or rocking back and forth during an attack. -
My neuro advised me to first see a cardiologist and have a contra-indication of doing the cold showers because my intake of verapamil is quite high and the cold may have an adverse effect on my heart. If you’re not on verapamil, by all means step into your budgie smugglers and have that ice cold water bath
-
You’re so right that the results have to come from the forums, as the results of the med trails are always statistical and most of the times not first hand by trail participants. I’ve been in the Aimovig trail in 2019 and Emgality trail in 2020. On both occasions trying to break my cycles as the meds (verapamil, naratriptan, sandomigran, prednisone, D3) I took were not sufficient anymore while the beast was jumping very ugly 8-14 times a day with kip 8-10 very often. I had 5 rounds of Aimovig and it did not break my cycle. It was only when I upped my verapamil from 600 to 720 that I noticed in hindsight brought the relief of ending my cycle. Aimovig had no side effects besides a minor obstipation. The Emgality I took last year also did not break my cycle, in fact this cycle started last year June and is still ongoing now for 11 months. I do not contribute that to Emgality, I believe the beast wants to ‘play’ with me a little longer than normal. I have to say that in my current cycle before I used the Emgality I had the GON injection which also has zero effect, but also no side effects. From the participants in both trail groups I understood that 4 of of 10 had positive results, their cycles did not start. Saying this, my observation is that those CGRP medicines are not meant to break cycles, it is to prevent them. Once in cycle there is little one can do apart from having your rescue meds on stand by and try to ride it out the best you can.
-
@kat_92 Fully understand that. The Aimovig is in the same order as Emgality here in the Netherlands, round 620 euro per shot. It is not covered by insurance though, so for me it would break the bank. I am chronic too and nothing really helps to get me out of cycle, but if it had been successful, i would seriously consider this, but both weren't. Hope you have PF days Alex
-
YALE STUDY- Psilocybin for the Treatment of Cluster Headache
Cast Iron replied to FunTimes's topic in General Board
And another Phase 2 trail on LSD. MindMed CorpUpdate 7.2.2020 -
Hi Kat, I was also in cycle when I tried Aimovig without any relief, but also without any side effects. This year I tried Emgality, again in full cycle, to no avail/side effects, just like Pebbles. These anti-CGRP meds may not work, or maybe are not strong enough to cancel out a cycle, but from what I read and hear is that it is intended as an preventive med. While I was in cycle my neuro and I actually hoped it could also work as an abortive to get me out of cycle, but in hindsight we both believe it is not designed that way. In the trail groups I was in, 4 out of 10 experienced the real benefits from it, preventing CH with just one round of shots every month. If there are no financial obligations, I would certainly participate in the trail, and hopefully you are out of cycle when you start. Alex
-
Hi Julie, Can you share some light on the signal pathway, as my understanding is that the enzymes in Emgality bond with the CGRP and therefore prevent that the CGRP can connect to the receptor causing/triggering the attack. Curious to know as Emgality did not work for me, nor did Aimovig. Alex
-
It was about a year and a half ago that I met the ‘kid’ on the video during a patient day in the neurological centre. Although his young age I was surprised how much he already knows about CH, but also that he was frank and open about the things science does not know yet. He said that O2 really helps, but they just do not know why?, is it because of the cold airflow up the nose, or that there is somewhere in our system a ‘switch’ that signals that enough O2 is in our blood and that the blood vessels can be contracted again. Anyway, they would like to start conducting scientific studies in a cross functional way, combining neurology between CH and Sleep, as they already highly suspect that there is an interaction between them. I said I would like to list for this because I am chronic, have severe OSAS and both my neuro’s also have the impression that these things tie together. Insomnia is a condition they know is related to this too. In the past years I’ve taught myself not to lie on my back as this blocks my airways in my sleep, I do have a custom designed dental brace that I wear at night to prevent obstructing my airways, but a CPEP can be used also if you suffer from apnea. Also during the weekend, my wife and children are watching over me not to fall asleep mid day as this will inevitably lead to a very rapid REM sleep and CH attack. Anyway, this young neuro is very ambitious and has the support of one of the leading neurological centres here in Holland. I do hope that in his lifetime he is able to crack the CH puzzle, maybe too late for us, but at least for later generations. Alex
-
Yesterday I heard from my neuro that SUN is working on a 3mg auto injector next to the normal 6 mg. Might be a possibility for folks that now have to split the 6 mg auto injector manually. Keep you posted on when it becomes available, here in Europe-Holland. All the best
-
Chronic and in cycle now for many months. I consider my cycle to be over when I can look strait into bright artificial lights without hurting my eye. In cycle I can look directly into the sun without eye pain, but not in artificial lights like car headlights on my cluster side. ATB
-
How to get prescribed more than 6 sumatriptan injectables a month.
Cast Iron replied to Mezzo's topic in General Board
In that respect I've made my way to the second level of hell, or possibly even further. My breakfast, lunch and dinner is consisting of verapamil, fravotriptan, sandomigran, paracoff, D3 regime to keep the Ch at bay. Agree that one should look for a good preventive other than the triptans. But you know, the beast behaves differently in every person, with different methods trying to keep it at bay. I am in a bad cycle now for 4 months, last month I've had 170 attacks, night and day. As another preventive I've had the GON injection (liquid prednisolone into the great occipital nerve), with no effect. The O2 will only take care of the smaller attacks, prednison will reduce the number and severity, but cant take them away fully. The number and severity is progressing rapidly, I have 10 attacks a day varying from kip 3-8, cant do the busting, last week started on emgality -have to wait for the first effects, if any as last year i had aimovig with no effect- so my last resort is the combination of O2 and 3-5 sumatriptans a day to not escalate it further into a kip 9/10. I know the hammer and rebounds are super big, but there is just no other way. Alex occipitnerve -
Hi Siegfried, is the remission period with or without medication, i mean can we be chronic in remission with medication that holds the beast at bay, or does it mean that remission is also without any medication? Alex
-
New to this forum – Cast Iron until hit by CH
Cast Iron replied to Cast Iron's topic in General Board
Hello Batch, Yes I do feel fortunate to live here, we have a combination of very old cities and hyper modern, its what visitors and tourists really can value over here. We are getting close to spring and than we have the wonderful fields of tulips again which are really photogenic: Many thanks for the time you've spent replying, next week I have a doctors appointment to determine the baseline through the lab tests. I already found the nutrients and going to order them. As soon as I have the lab results I will chime in again. Best regards!
-
Hello SPP-Fan Welcome to this forum, although not good that you have found it as CH cluster headache is a serious thing if you have it. My first thoughts are to see if you have one or more of the following signs or symptoms: Excruciating pain that is generally situated in, behind or around one eye, but may radiate to other areas of your face, head and neck One-sided pain Restlessness Excessive tearing Redness of your eye on the affected side Stuffy or runny nose on the affected side Forehead or facial sweating on the affected side Pale skin (pallor) or flushing on your face Swelling around your eye on the affected side Drooping eyelid on the affected side Diagnoses of CH is done by eliminating possibilities while taking into regard the above symptoms. Especially the first and second may be a first indication for cluster headache, along with a one or more of the others. People experience sometimes different signs because CH can morph over the years, but as a starter you can see if the above applies. Seriously hope it is not CH and take care the next time you have sex.
-
FT..you may want to continue with the Emgality for a while more as the body needs to learn that the anti-CGRP fits the CGRP receptor and thus can block the binding of the CRGP to the receptor when the CGRP is released by the body. Some body's will learn this within a couple of weeks, for others it will take up to a couple of months. I've been on a similar med Aimovig for 5 months with no result -instead I went up to 170 a month-, while luckily for others it proved to be helpful after 3-6 months. My last resort is also lithium, but this is really scary stuff. If I would take it, my neuro advises to first start a tapper of prednison, slowly increase the lithium (have your blood monitored constantly), while also decreasing the verapamil until you reach an equilibrium (CH have reduced or more or less stable in number of attacks), and then increase lithium slowly further and lower the verapamil to zero. By then the prednison can be reduced to zero. The whole process may take quite some time and for a good reason as my neuro stressed that suddenly stopping verapamil and starting lithium generally gives very adverse effects. It may turn out that if this occurs, returning back to verapamil, even in high doses, does not give the same result as before. All the best