Leaderboard



.thumb.jpg.24dde7ef3152d6d31b9546e3fec3b26d.jpg)
Popular Content
Showing content with the highest reputation on 07/05/2019 in all areas
-
Hey batch, I meant what I said you do a great service to the community. I have directed many people to D3 and your work. It was just the opening statement that got me. Keep up the good fight. Brian2 points
-
Hey Freud, Fair comments about my post to JH. Too much bravado and not enough factual data... I've fixed that with an edit. Take a look and let me know if it passes muster. Regarding the online survey data, I've kept my reporting of that efficacy data as objective as humanly possible. I'll be happy to show you the survey database this coming September at the Clusterbuster Conference in Dallas, TX. Credibility is everything when talking about efficacy of a CH intervention like Vitamin D3, so I'm not about to risk that credibility by making false, misleading or exaggerated claims. I've too many neurologists, headache pain specialists, vitamin D3 experts, CHers and a growing number of migraineurs following my work. A few neurologists have even been kind enough to provide peer reviews and feedback... Two of these neurologists are CHers so are taking this vitamin D3 treatment protocol to prevent their CH. For reference and for those who don't know me, I'm a 74 year old retired Navy fighter pilot with over 3000 hours flying Navy fighters. I have a dated degree in Chemistry circa '67 from the University of Washington, I've been a CHer since 1994 and diagnosed as chronic by neurologists at NIH in 2005. I'm not a doctor so I don't diagnose, prescribe or treat CHers or migraineurs. What I do is provide information outreach on safe and effective non-pharmaceutical CH and MH interventions (O2 and Vitamin D3). That information is based on feedback data from thousands of CHers I've been collecting since September of 2006 on CH.com with my first posts on the benefits of oxygen therapy with hyperventilation as a CH abortive, on 10 December 2010 when I began posting about my experiences preventing CH with vitamin D3 and the cofactors as well as detailed data from the online survey of 293 CHers following the anti-inflammatory regimen CH preventative treatment protocol to prevent their CH. This survey went online over the Internet in January of 2012. When asked for suggestions or answers to CH related questions about this treatment protocol, I generally provide answers based on what many other CHers or I have found. I also suggest CHers and migraineurs see their PCP/GP or neurologist to discuss the anti-inflammatory regimen and to obtain the essential lab tests for serum 25(OH)D, calcium and PTH. I don't sell anything, nor have I taken one cent in renumeration for any of my posts about the benefits of vitamin D3 in controlling CH and MH here at Clusterbusters, over at CH.com or on Migraine.com... My wife will attest to that fact as she does our books. She frequently points out that I've spent an average of $2,500 a year (out of pocket) since 2006 providing information outreach to CHers and MHers on the benefits of oxygen therapy with hyperventilation as well as the benefits of vitamin D3 and the anti-inflammatory regimen in preventing CH, MH and in promoting improved health since December of 2010. I even spent two weeks in early 2018 posting in Facebook CHer and Migraineur groups. I got booted off Facebook after a couple posts on the effectiveness of the anti-inflammatory regimen in preventing migraines. It appears Facebook's Big Pharma sponsors didn't like what I posted so had me blocked. I've been paying $100/year to keep online survey running since 2012 and my annual dues as a member of the American Academy of Neurology (AAN) as a vitamin D3 and Cluster Headache researcher have cost me $260/year since 2013... My annual travel, lodging, meals and registration costs to attend conferences, meetings with neurologists and to make presentations on the effectiveness of oxygen therapy with hyperventilation and the anti-inflammatory regimen since 2009 have averaged $2,000/year. I've made two trips to Switzerland, two trips to Norway and one trip to Germany to attend meetings with fellow CHers at CH conferences and to meet with neurologist like Prof. Dr. med Ottar Sjaastad in Haugesund Norway, Prof. Dr. med. Arne May at his headache clinic at the University of Hamburg Eppendorf (UKE) Germany and Dr. Todd Rozen, MD, FAAN at his facilities in Wilkes-Barre PA. If you'll check the fine print in the ICHD-III beta website, you'll find Dr. May and Dr. Rozen are in the working group responsible for trigeminal autonomic cephalalgias. Dr. Rozen was kind enough to stop by my poster presentation on results from the online survey of CHers taking the anti-inflammatory regimen at the 2014 AAN Annual meeting in Philadelphia, PA. The reason for the Cowboy getup is simple... I grew up on a horse and during my poster presentation, I didn't want anyone thinking I was a neurologist. What most people don't know is I've been quietly going down the rabbit hole in search of answers that will help me define a more detailed pathogenesis of CH and MH as well as determine how and why vitamin D3 and its conutrients/cofactors are so effective in preventing CH and MH. I track all vitamin D3 RCTs as well as cluster headache and migraine RCTs on clinicaltrials.gov and weekly editions of the AAN journal Neurology. This research has taken me into the realm of molecular biology and gene mapping. There are quite a few neurologists doing this kind of research using anti-CGRP monoclonal antibodies as CH and MH prophylaxis, but none using vitamin D3 as a CH or MH prophylaxis. I'm a member of PLOS - a nonprofit publisher innovator and advocacy organization, the Cureous journal of medical research, and Researchgate where leading edge studies and scientific papers like this are published. That said, there are a growing number of physicians now trained in the Coimbra vitamin D3 protocol for preventing multiple sclerosis. Dr. Coimbra has treated over 2000 of his multiple sclerosis patients with his vitamin D3 protocol and his patients have a 95% complete remission rate. So why am I doing all this? It's clearly not for the money... It's also not an ego trip seeking credit for the many findings made public about the safety and efficacy of oxygen therapy with hyperventilation as a CH abortive or the anti-inflammatory regimen as a safe and effective CH prophylaxis... That credit goes to the thousands of CHers who took the leap of faith to try these two CH interventions then took the time to provide their feedback. That feedback is what motivates me to keep doing this as I know the terrible disabling pain of our disorder and that the good news is it doesn't need to be that way. By the way, I'm a strong supporter of CHers using psilocybin or seeds as a safe and effective CH prophylaxis. The data I've collected to date from CHers here at Clusterbusters indicate the vitamin D3 protocol and psilocybin treatments are not mutually exclusive. Although the data is largely anecdotal due to small numbers, It appears these two CH prophylactic treatments have a synergistic effect when taken together. Take care, V/R, Batch2 points
-
1 point
-
This sounds like a situation that is sometimes described here. A reason to give indomethacin a fair try with treatment-resistant symptoms that seem to be CH. https://www.docguide.com/case-remitting-hemicrania-continua-seasonal-variation-and-clustering-diagnostic-confusion-cluster-he?tsid=5 A case of remitting hemicrania continua with seasonal variation and clustering: a diagnostic confusion with cluster headache (May 2019) Hemicrania continua (HC) is an indomethacin responsive primary headache that is characterised by a continuous strictly unilateral headache with periodic exacerbations. About 15% may have a remitting subtype of HC. Herein, we are reporting a 36-year-old man who had a 5-year history of episodic right-sided headaches. The headaches used to occur in a discrete series lasting 4-6 weeks, separated by pain-free remissions of 10-11 months. In each relapse, he had continuous background pain with superimposed exacerbations. The superimposed exacerbations were 1-2 attacks per day, lasting for 2-5 hours, and were associated with ipsilateral cranial autonomic symptoms. However, the patient did not respond to usual therapies of custer headache (CH). He had a complete response to indomethacin. We suggest that remitting subtype of HC may mimic CH. A therapeutic trial of indomethacin should be done in all strictly unilateral headaches that are not responding to other drugs.1 point
-
This! This is exactly what I've been experiencing as I've been tapering off of Verapamil. Stomach all knotted up, felt like I most certainly needed to visit the toilet to purge from somewhere, nope. Chest real heavy, get the sensation like I'm running out of breath. I check my Fitbit heart rate monitor and it's at 70-110 bpm while at rest. The sensation continues to build into an attack. It happens every time preceding an attack now My normal resting heart rate is 55bpm.
 1 point
1 point -
Hope you don't have to wait till September for relief, sounds like this isn't your first rodeo and nobody knows ur body and cycle better than you. Good luck!1 point
-
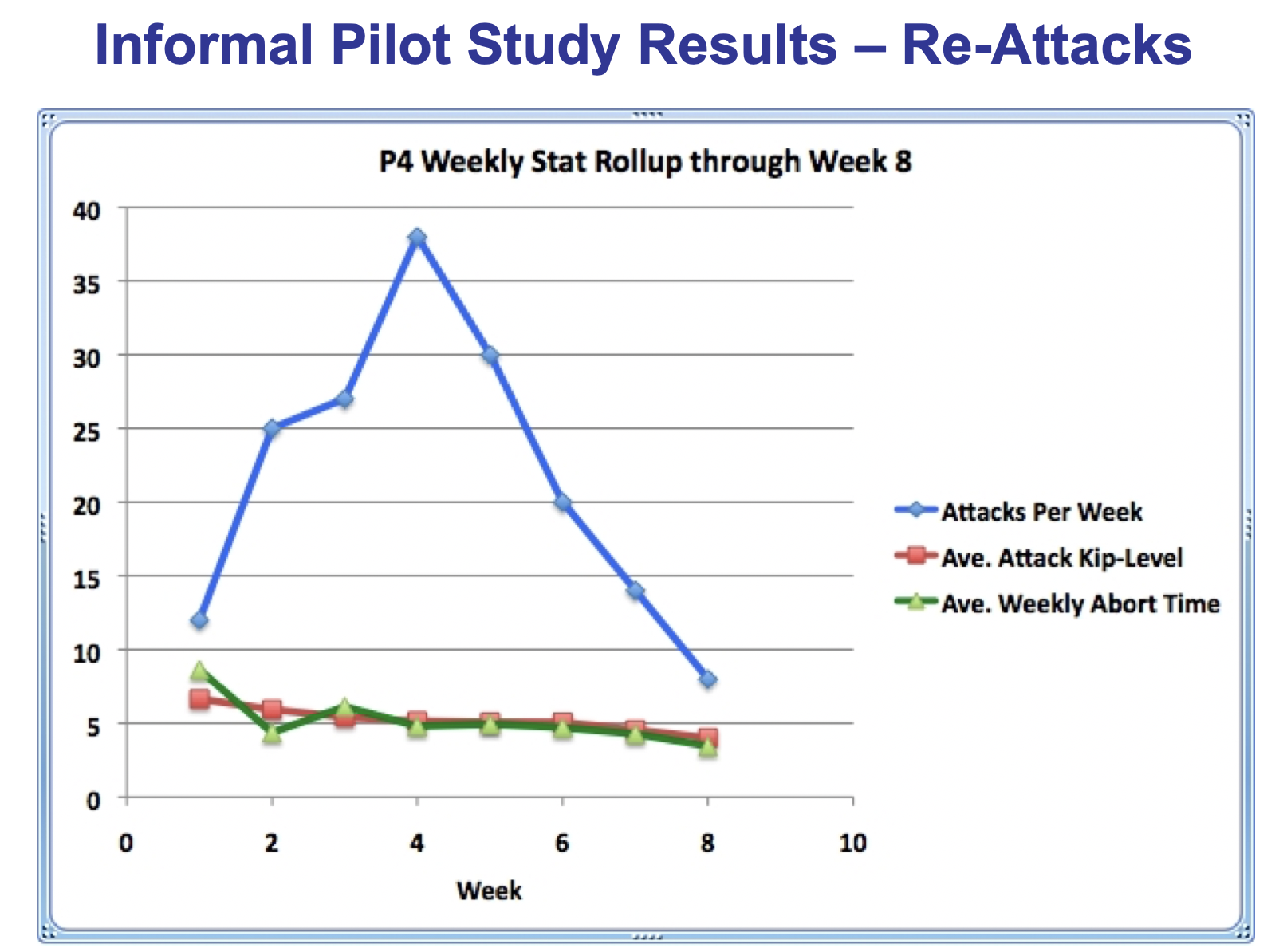
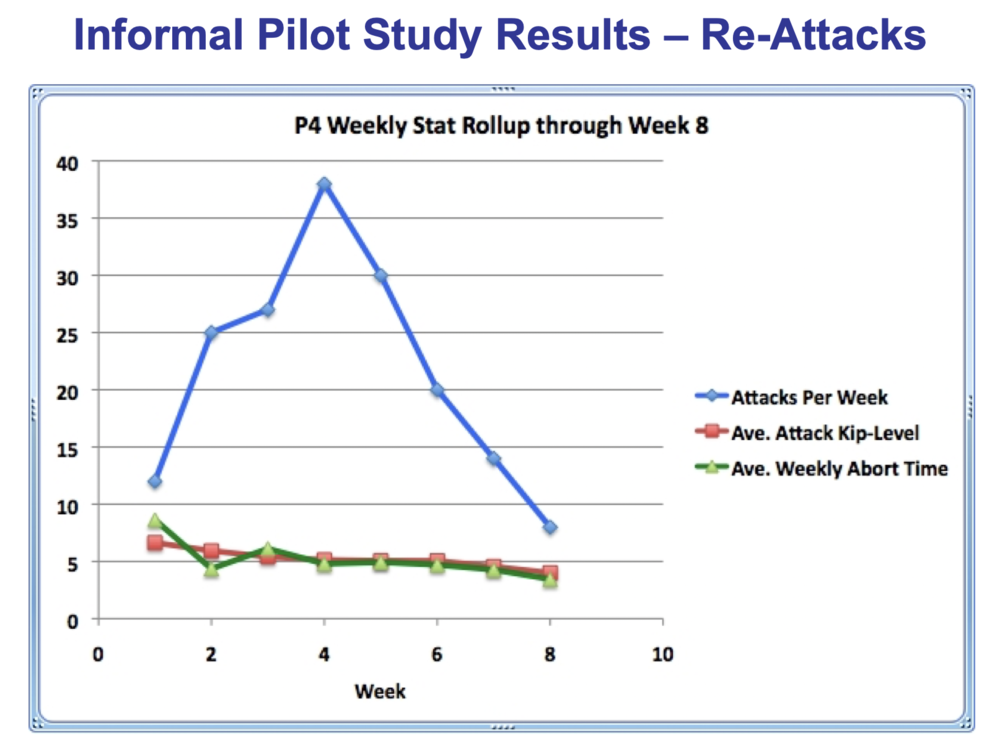
Hey THMH, Great answers and assessment. I'll add to your comments. In 2005 after turning chronic, I developed a method of oxygen therapy that supports hyperventilation. It used oxygen flow rates between 25 and 40 liters/minute and resulted in average abort times around 7 minutes and better than 95% effective in terms of successful aborts over total attempts. Abort times this short and efficacy were clearly better than that obtained at a flow rate of even 15 liters/minute. I started posting about my experience with this new method of oxygen therapy on CH.com and was told by many that oxygen flow rates this high was dangerous... Well... As a Navy fighter pilot with over 3000 flight hours in Navy fighters breathing 100% oxygen from takeoff to landing (usually aboard ship) on every flight and at very high respiration rates during high G-Force maneuvers during practice and actual combat maneuvers... I knew oxygen flow rates this high were very safe... or I wouldn't have passed my annual flight physicals with PA and Lateral chest X-rays. In 2007, I received an oxygen demand valve from the Linde Group subsidairy here in the US so modified my initial oxygen therapy procedure and breathing techniques to work with the oxygen demand valve. It worked so well I decided to set up a pilot study to capture efficacy data in terms of time to abort by pain level. We conducted the pilot study of the oxygen demand valve method of aborting CH in 2008 with seven CHers (6 CCH, 1 ECH) each recording the pain level at start of therapy and time to abort for every CH over a period of 8 weeks. In all, they collected data on 366 aborts. This method of oxygen therapy required intentional respiration rates that support hyperventilation roughly equivalent to an oxygen flow rate of 40 liters/minute. The breathing procedure used with the oxygen demand valve method of aborting CH (DEVO2) is far from passive. It's hard work huffing and puffing like a big dog with respiration rates up around 20 inhalation-exhalation cycles/minute at forced vital capacity lung tidal volumes. The initial pilot study protocol called for a week of aborts at an oxygen flow rate of 15 liters/minute with a non-rebreathing oxygen mask as a comparative then switch to the oxygen demand valve for 8 weeks. However, after the first participant completed the week at an oxygen flow rate of 15 liters/minute and switch to the oxygen demand valve, his abort times dropped so dramatically, we scrapped the comparison phase and went straight to the oxygen demand valve phase for the remaining six participants. The primary efficacy endpoint for this study was an abort with the oxygen demand valve in 20 minutes or less. The following graphic illustrates the efficacy results in time to abort by CH pain level. 364 aborts met the primary efficacy endpoint. The two aborts that failed to meet the primary efficacy endpoint involved the same unlucky participant who got trapped away from his demand valve system until his CH had already reached a 10 on the 10-Point Headache Pain Scale. He was out shopping when one CH hit and got locked out of his house on the second. These two attempts were technically no-tests due to the delay in starting oxygen therapy, but I elected to count them anyway. This made the efficacy of the demand valve (DEVO2) method of aborting CH 364/366 or 99.4%. No other known CH abortive is this effective. As you can see, the DEVO2 method also produced CH aborts 3 to 4 times faster than aborting CH a flow rate of 15 liters/minute. The mean abort time for the 364 successful aborts was 7 minutes across pain levels 3 through 9. You'll also notice that the abort times increased with CH pain level at start of DEVO2 therapy. This is reason enough to start oxygen therapy at the first sign of an approaching CH. Regarding the change in CH frequency after starting oxygen therapy, the following chart illustrates the change in CH frequency measured in CH attacks per week over the 8 week period each CHer used the DEVO2 method. We called this up-tic in frequency of CH Re-Attacks for the simple reason Medication Overuse Headache (MOH), also known as rebound headache doesn't really apply to oxygen. MOH are more frequently associated with repeated longer term use of opioids, analgesics, triptans and NSAIDs. In addition, oxygen toxicity is not a factor for the period and total time spent breathing 100% oxygen as a CH abortive at normobaric pressure. The increase in Re-Auttacks (up-tic in CH frequency) up to week 4 appear to be caused by a number of factors including an incomplete abort (staying on oxygen breathing normally for 5 to 10 minutes after the pain stops helps increase the time between CH), speed of abort and relatively short physiological period of efficacy (effects wear off in 30 to 45 minutes after returning to normal respiration rates with room air). If CH triggering mechanisms are still active, CH return in 1 or 2 hours. The decrease in CH frequency between week 4 and week 8 is an interesting phenomenon. We think this is due to vascular toning... In other words, the muscles lining the arteries, capillaries and micro vasculature get stronger or tone up with repeated flexing (vasoconstriction) during DEVO2 therapy. This is similar to doing pushups or lifting weights. The more frequently you do these physical activities, the stronger your muscles get... In short, you've toned them up. Although this up-tic in CH frequency between week 1 and week 4 was irritating, the reduction in average weekly CH pain level and and average weekly time to abort over the 8 weeks was continuous. All study participants viewed this initial up-tic in CH frequency as acceptable given the overall high efficacy and speed of abort using DEVO2. The mechanism of action behind the high efficacy and short abort times for the DEVO2 method of aborting CH involves intentionally hyperventilating with 100% oxygen at effective flow rates of 40 liters/min. This blows off CO2 from the lungs faster than the body generates it through normal metabolism. This elevates blood pH (makes it more alkaline) and that elevated pH increases blood hemoglobin's affinity for oxygen allowing it to upload more oxygen and offload more CO2 more rapidly (Bohr effect). The increase in hemoglobin's affinity for oxygen results in a super-oxygenated flow of blood to the brain at roughly 115% of that obtained breathing room air. This results in a very rapid vasoconstriction of the trigeminovascular system which acts as one of the CH abortive effects. This increased blood oxygen super-saturation also results in Calcitonin Gene-Related Peptide (CGRP), Substance P (SP) and Vasoactive Intestinal Peptide (VIP) being metabolized much faster, lowering their cellular concentrations and that increases the CH abortive effect. CGRP, SP and VIP have all been found elevated in serum concentrations during the pain phase of CH and migraine headache (MH). There are three related factoids to consider. The first factoid is although the numbers are limited, the DEVO2 method and procedure of aborting CH appears to be just as effective in aborting migraine headaches. The second factoid is the latest method of oxygen therapy I developed in January of 2010 involving intentional hyperventilation with room air at forced vital capacity tidal volumes for 30 seconds followed by inhaling a lungful of 100% oxygen and holding it for 30 seconds then repeating this sequence until the CH pain is completely gone results in the same CH abort times (an average of 7 minutes) and efficacy as the DEVO2 method. This method of oxygen therapy consumes one tenth the volume of oxygen as the DEVO2 method. This brings the volume of oxygen consumed per CH abort down from 250 to 300 liters to 25 to 30 liters. That works out to a reduction in oxygen cost per abort from one dollar/abort with DEVO2 down to roughly 15 cents/abort with this new method. The third factoid... The anti-inflammatory regimen with 10,000 IU/day vitamin D3 plus the vitamin D3 conutrients is so effective as a CH prophylaxis, my collection of oxygen therapy hardware costing more than $2,500 has been sitting in a storage room, untouched since October of 2010 when I started this vitamin D3 regime. The following graphic illustrates the favorable response rate by day after start of regimen. I estimate over 2000 CHers and many migraineurs have started this regimen since I began posting about my experiences with it on CH.com in December of 2010. This is a conservative estimate as readers of my webpage at the following link http://is.gd/clustervitd on VitaminDWiki.com have downloaded 17,727 copies of the anti-inflammatory regimen treatment protocol since 21 January of 2017. That works out to a little over 22 downloads a day. I'd also like to point out the anti-inflammatory regimen works well with busting. In fact, when taken together they appear to have a synergistic effect in preventing CH. So there you have my 75 cents worth of comments on oxygen therapy... I welcome any comments. Take care, V/R, Batch
 1 point
1 point