Leaderboard



Popular Content
Showing content with the highest reputation since 01/27/2026 in Posts
-
Welcome to the community @Nikola, sorry you have the need to join us!! Unfortunately, the short answer is there really isn't a definitive answer to your question!! ive been a episodic clusterhead since 84.....42 glorious years now......before I got here 16 years ago my cycles we're fairly predictable.....18 to 19 month remission and 5 to 6 mo cycle usually beginning in August. But I know many folks that get 2 cycles per year and always have.....the untreated Beast truly has a mind of it's own!! Couple things you might look at here are high flow oxygen for aborting individual attacks, and the anti inflammatory vitamin D3 regimen to lessen the frequency and severity of attacks. Dallas Denny5 points
-
Hi @CHfather and @dhuddly. Sorry you find yourself in our company there dhuddly, I haven't been on past couple weeks with some life changes I alluded to above and a number of projects on the go. I would appreciate links to studies you've read, always keen to expand my knowledge of the vitamin D3 literature. Here are the studies and their findings relating to the dopaminergic system in CH published last year for your reading and interest. What I would say above and beyond these studies, the work that has come out over the past number of years in CH space makes it fairly clear that between the active bout periods in episodic CH, the patient does not return to a normal baseline, the attacks may stop but there are perturbations that extend into the interictal periods that give me some level of assurance that I am doing the right thing for myself in terms of staying on the anti-inflammatory regimen 365 days of the year. I also hope that in doing so, I am providing an additional level of protection against developing other disease. I have more recently revisited Dr. Gominak's work (a contributor in part to the regimens inclusion of the B-Vitamins) and believe another reason for the regimens efficacy relates to vitamin D3's influence on the composition of the gut microbiota and the maintenance of epithelial tight junctions. Given nearly every cell expresses the VDR and the lack of formal studies in CH, it would be impossible for us to confirm Pete Batcheller's original hypothesis as to its precise mechanism of action (and as you mention, partial or non-response) but I think he is on the money with the umbrella thinking that it's underlying mechanism is the up and down regulation of genetic products which have the VDR sequence in their promoter / enhancer or silencer regions on DNA. Dysfunctional mesocorticolimbic circuitry in cluster headache. Ferraro et al. (2025) This fMRI study used a "Monetary Incentive Delay" task to probe the mesocorticolimbic dopaminergic pathways. Chronic CH (cCH): Patients exhibited blunted activity in the Ventral Tegmental Area (VTA) - a central dopaminergic hub - during reward anticipation. They also showed an imbalance in the pathway between the VTA and the medial prefrontal cortex (mPFC). Episodic CH (eCH): Patients showed intact VTA responses but abnormal mPFC activity, which the authors suggest may be an early sign of emerging dysfunction in the VTA-mPFC dopaminergic pathway. Conclusion: The study suggests an abnormal dopaminergic state in chronic patients that is distinct from affective disorders (depression/anxiety). Uncovering the neurological substrates underlying restlessness in cluster headache - A functional MRI study Chen et al. (2025) This study investigated the neural correlates of restlessness/agitation, a core clinical feature of CH. Substantia Nigra (SNpc): Patients experiencing restlessness showed increased functional connectivity between the Substantia Nigra pars compacta (SNpc) - a dopamine-producing nucleus - on the pain side and the Locus Coeruleus (noradrenergic) on the non-pain side. Frontal Inhibition: The study found decreased connectivity between the pain-side SNpc and the superior frontal gyrus, suggesting a disruption in top-down inhibitory control contributes to motor restlessness. Neurotransmitter Imbalance in Cluster Headache: A Systematic Review of Mechanisms and Therapeutic Targets Pellesi et al. (2025) This review aggregates data from multiple biochemical studies regarding dopamine levels in CH. Platelet Levels: Citing D'Andrea et al. (2006), the review notes that platelet dopamine levels were significantly higher in patients with episodic CH during both active bouts and remission compared to healthy controls. Plasma Levels: Citing D'Andrea et al. (2017), the review reports that patients with chronic CH exhibited higher plasma levels of dopamine compared to controls. Cerebrospinal Fluid (CSF): Citing Strittmatter et al. (1996), the review notes that CSF levels of dopamine were not significantly different between CH patients and controls, though norepinephrine was reduced. Autonomic dysfunction in patients with episodic cluster headache during remission period López-Bravo et al. (2025), This study summarizes previous biochemical findings in CH. It cites D'Andrea et al. (2017) regarding Abnormal Tyrosine Metabolism: Chronic CH patients show increased levels of dopamine and its precursor tyrosine in plasma. The authors interpret this anomaly in tyrosine metabolism as a potential predisposing factor for the chronification of episodic CH. Thesis: Felicia Jennysdotter Olofsgård (2025) Jennysdotter Olofsgård (Thesis) Genetics: A meta-GWAS identified WNT2 as a new risk locus for Cluster Headache. The author notes that WNT2 is known to be involved in dopaminergic neuronal development. What is seldom discussed in our community is the psychological and personality dimension of CH and how that relates to this topic. Kudrow and Graham were notably candid in the 1970s. I hesitate to be quite so direct, yet many of the personality characteristics they described feel uncomfortably familiar, as though my name might as well have been written beside them. If I may delicately say @dhuddly, from your posts and your manner of written expression, you come across as highly intelligent, thoughtful and kind. You have also mentioned being a full stack developer (I saw that response on a possible CB app - thank-you!), someone your friends describe as operating at extraordinary speed. I want to be clear that I am not attempting to analyse or explain you, rather, those observed qualities deeply resonate with me and provide a useful reference point for describing how I have come to interpret similar tendencies in my own life, over-achievement, high intelligence, tendency to work at a million miles an hour to name but a few. So... here's my story and my take on those qualities in the context of my life journey and CH. My father died before I was born. Throughout childhood I struggled to understand, let alone regulate, the emotions associated with that absence. In adolescence this unresolved grief drifted into substance abuse. Later, the same undercurrent appeared to transform into an intense drive for achievement, knowledge, and ultimately explanation. A life organised around such a pursuit rarely tolerates stillness. Pausing to enjoy simple pleasures can mean confronting emotions one has never properly learned to process. I am still learning how to do that. My sense, shaped by both experience and reading, is that unprocessed anger, grief, and guilt can sustain a chronic autonomic bias toward fight or flight, with downstream effects across our physiology. Viewed through that lens, it is perhaps unsurprising that my nervous system, which has otherwise been remarkably resilient, shows points of vulnerability. I cannot claim definitive evidence that CH, or another unique and uncommon disorder I am afflicted with - vocal cord dysfunction, arises from such experiences. This remains an interpretation, not a conclusion. The closest conceptual framework I have encountered is found in the work of Dr Allan Abbass, particularly his writing on overcoming emotional resistance through Intensive Short Term Psychodynamic Therapy. I feel his work and this topic deserves more discussion, as confronting as these topics can be. Link. Anyway, I pray I have not overstepped and I welcome you here with open arms. I am glad to connect. Craig.3 points
-
Hallo! Currently operating on an available budget of £5K, but aiming for £15-20 total, to cover the full process including post-prod, and festival submission etc... Initially, we were planning to run it on the shoestring/low budget end of things, but my new director is keen on securing proper funding so we're not compromising on quality or fees. We have a possible producer on board now and links to a few potential backers, but all interest is good interest! The script is currently 14 pages and we'll be aiming at 10-12minutes or so Cheers!3 points
-
Hey folks, my name is Knyaz, who want to make more easy our lives and i have created "Migraine Tracker: Relief Pain" app which is serve for us. I need your help and feedback what i should add or delete pelase help me. App link: https://apps.apple.com/pl/app/migraine-tracker-relief-pain/id6755659669 WebSite: https://www.migraine.live/2 points
-
The above app is 100% hosted and stored on your own phone/tablet. No data is transmitted to anywhere else. I specifically built without Google play services for privacy reasons. Now to be honest I would not install a random app on my device without knowing where it came from. So my recommendation is to load it on a old phone you got kicking around and try it there first. It won't need a sim card or even to be up to date, and can be installed over wifi.2 points
-
I wish I had never started the Verapamil to begin with. I was put on it and was up to 1080 mg a day. Side effects sucked for me, not being able to feel from my knees down and swollen feet all the time. I took myself down to 120 twice a day without any change in my cluster frequency or pain level. I think the doctor I had at the time just had no clue and kept upping the dose. I finally was able to come off the verapamil after 10 years due to a newfound treatment. The D3 protocol is a cleaner option and I feel that I have benefited from that a little more that the Verapamil. @Crispo follow CHfather's post and links he will not disappoint!2 points
-
Hi @Nikola, I've probably made mental note of this especially since it corresponds to my own experience, but I've seen many report extending remissions as their decades with CH hurl by. In fact for nearly a couple decades, remissions between my bouts with episodic CH (which started around 1980) were ever-increasing in length, something I imagined that if I'd kept track, those extensions might have correlated to some sort of Fibonacci number series. The bouts themselves extended also though, increasing in length from a couple weeks to 2.5 months, and at some point the attacks increased in severity, with the individual attacks going on as long as 3 hours, compared to maybe 20 minutes or so with my very first inaugural attacks. This increased-severity deal could have been spurred by one truly honking drug cocktail I was prescribed at a point, though imitrex, the most oft-accused drug for causing such issues, wasn't even available then. I still find myself with nice longgg remissions, but not predictably ever lengthening - I've had shorter ones following longer ones, so no pattern anymore. The blue 'New Users Read Here First' banner up top of the page here ^^^^^ provides introduction to the manner in which many of us have successfully thwarted the Cluster Bunny when it comes a 'knockin, and the Basic non-busting information is good too:2 points
-
Hi folks! I'm an actor and writer living in London, and I have written a short film about living with Cluster headaches. It's based entirely on my own experiences, though descends into some more abstract representations of the pain, for which I've taken inspiration from forums and conversations with other sufferers. Currently it doesn't delve into 'busting' though if I can get it made, I may well pitch for a second or a series. It's called 'Clusterfu*k,' and I have a director on board and the beginnings of a budget as well as some locations and talent. Basically, I'm wondering if anybody knows of any organisations or individuals who would be interested in helping support, endorse and/or finance the film? I have a number of contacts in the screen industry and my new director is very well connected, but as with all arts at the moment, funding is going to be the sticking point. For me the film is an attempt to visually communicate the difficulties, pain, and sometimes amusing quirks of living with this illness and trying to get on with life. Overall, I've been relatively fortunate in my response to medications (verap, O2, Triptans etc), while living in the UK means I have access to NHS oxygen, which is a gamechanger. I guess I'm hoping to raise some awareness, communicate the actual experience of the headaches (which often feels near-impossible and a stumbling block for future engagement/research) and create a platform for myself as an artist. Let me know if anything jumps to mind, or if anyone is particularly interested in talking about it further. Enormous thanks and solidarity, Angus2 points
-
"Completely CH free" isn't what everyone on the D3 regimen achieves, but glad you've arrived there!2 points
-
I must of missed them, I've had 20-25% results with busting, I'm on the D3 regime all the time, I thinks its just good health to be anti-inflammatory, I also intermittent fast to keep inflammation and insulin spikes down. I tried a 96 hour fast at the beginning of this cycle, and so far I think its reduced overall attacks. I'll try anything during a cycle. But once its gone, I rarely even think about it.1 point
-
Herbal cigarettes may be tobacco-free and nicotine-free, but they still produce smoke when burned, and that smoke can irritate the airways and potentially trigger coughing, wheezing, or asthma-like symptoms in sensitive individuals. “Herbal” does not automatically mean safe for the lungs. If you’re curious about the types available in the market, you can explore this list of herbal cigarette brands. However, even these product can still cause repiratory irritation, beacuse the main issue is the smoke itself, not the tobacco.1 point
-
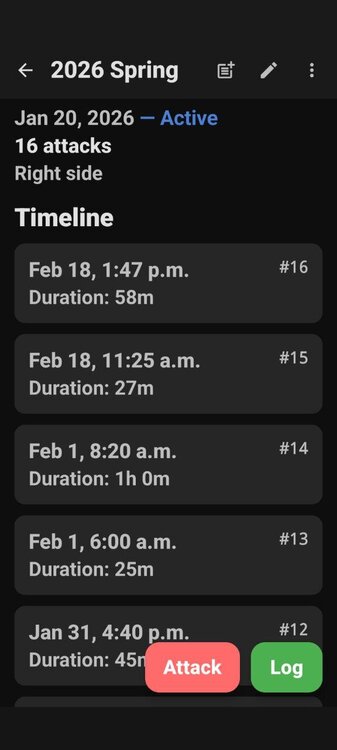
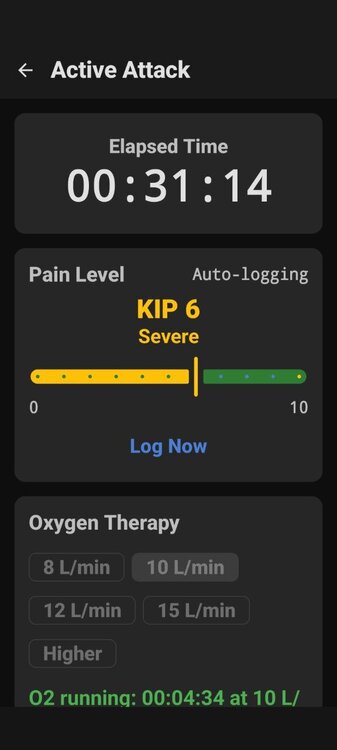
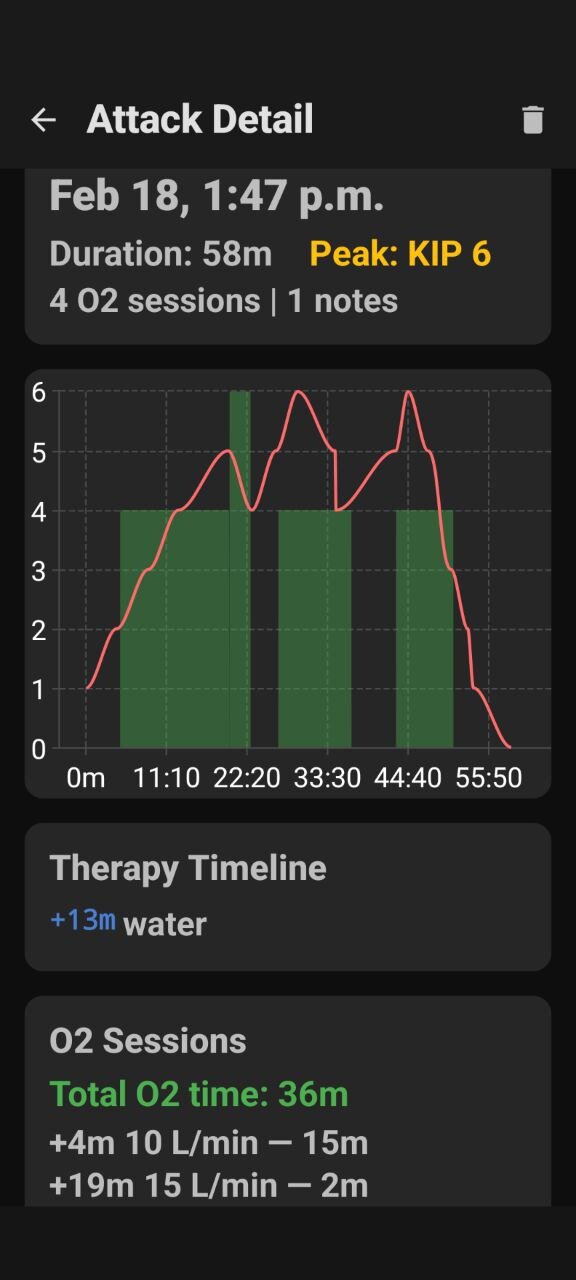
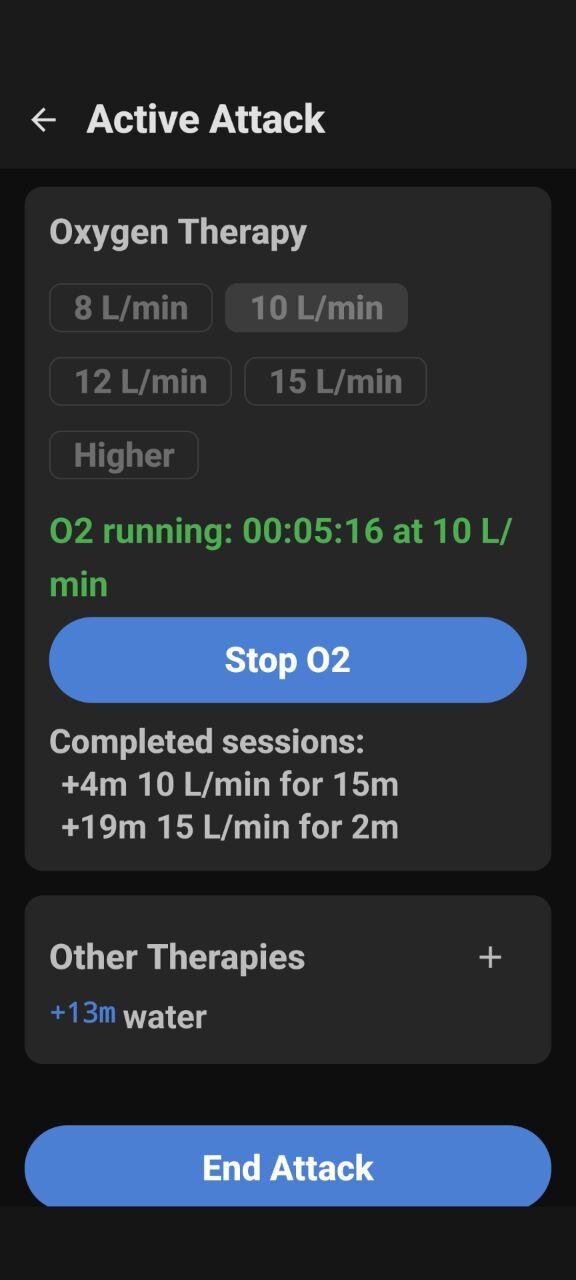
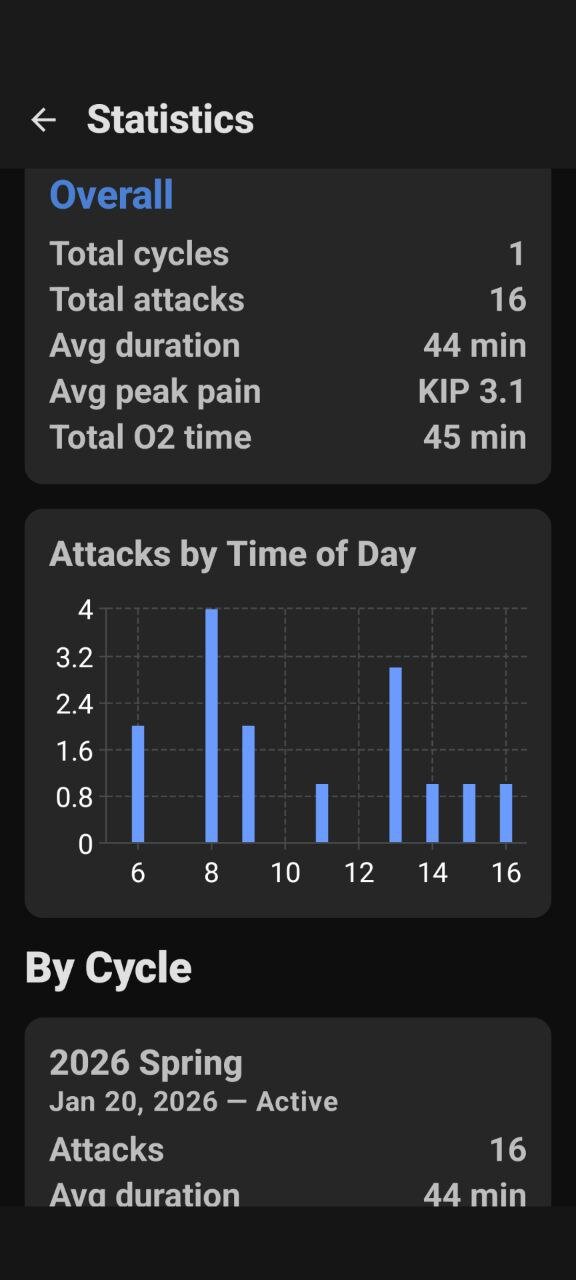
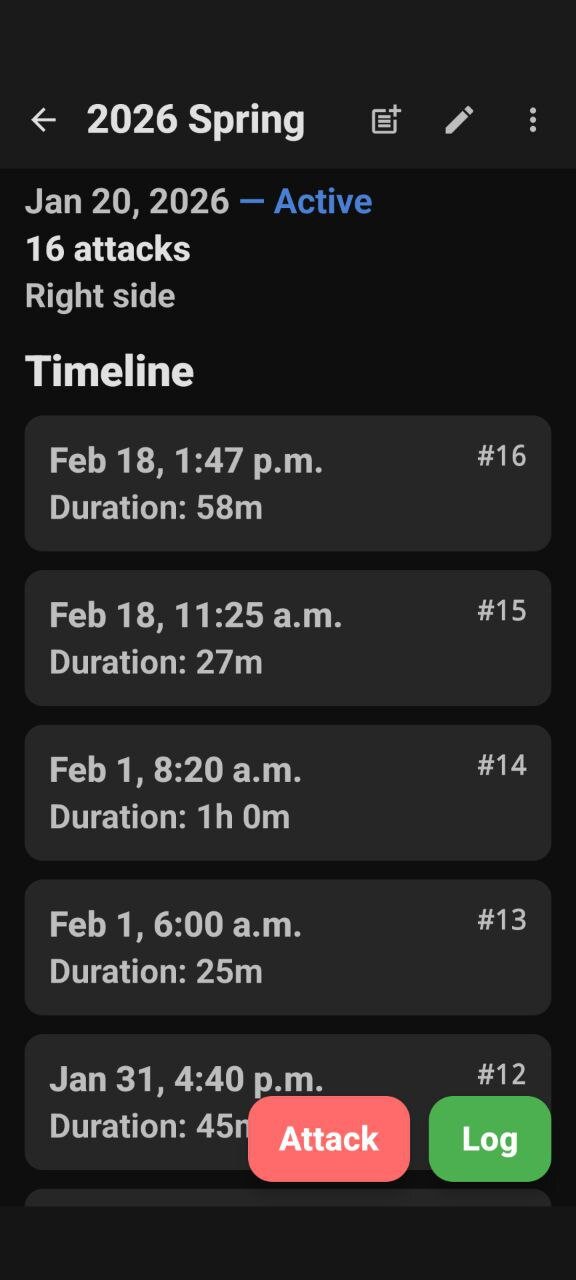
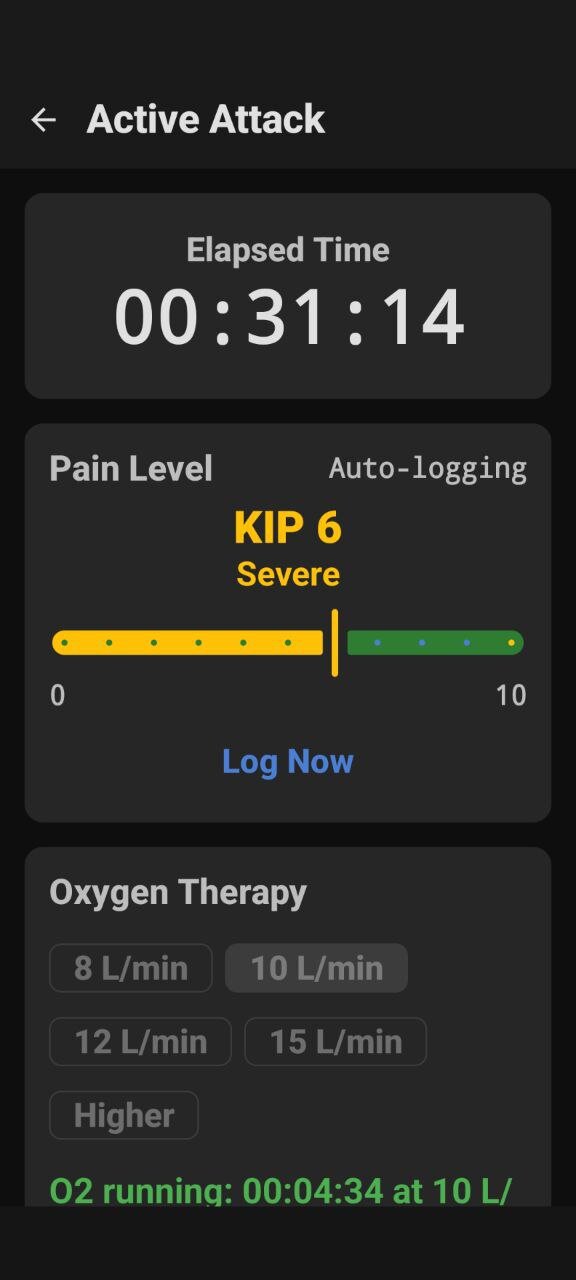
Here is some screen shots, also of note not available on i-phone. You can see where I thought it was going away, so I stopped O2, then quickly regretted that.
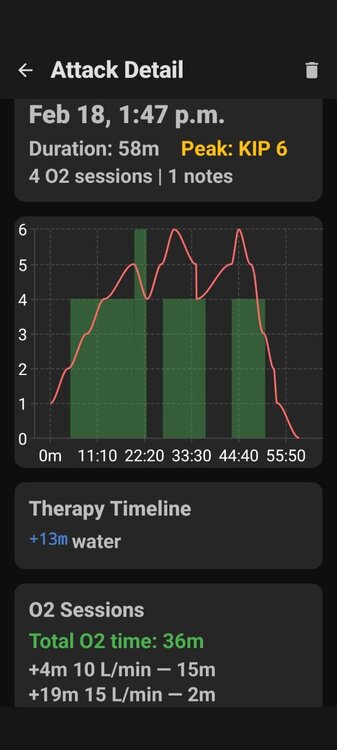
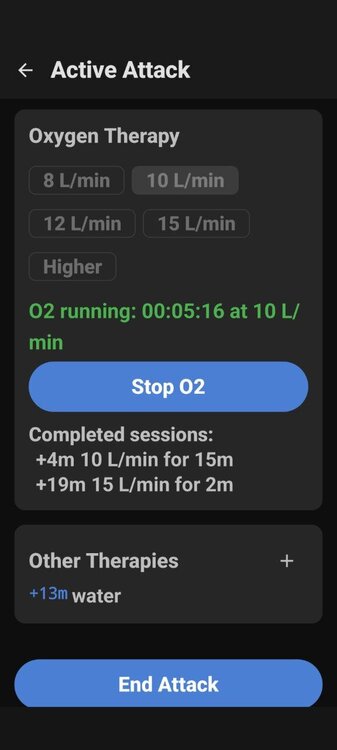
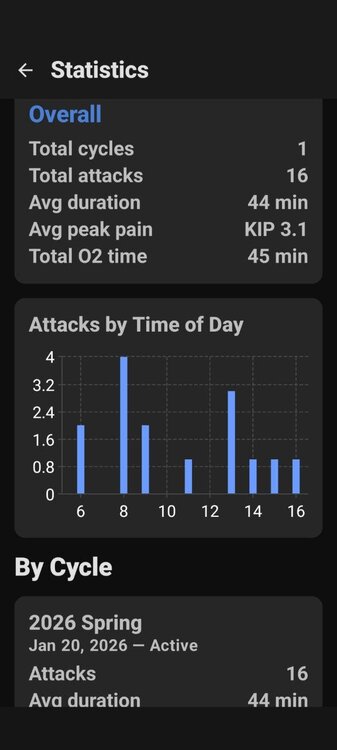
 1 point
1 point -
Its got some minor glitches I am still working out but here is what I built for myself. I use it to track cycles, attacks within the Cycle and the attack it self. If there is interest I will provide updates. The glitches I found where adding past attacks, the calendar was off by one day, so I choose one day ahead for yesterday's log date. I also want to add the ability to edit past attacks and notes. But otherwise working great. Provides good analytics for Cycles, and Attacks. Logs Pain, and O2 Usage and tie to local weather for increased data collection. Files can be exported into JSAN or CSV for medical or historical record keeping. The Notes can be for anything you wan to record, busting attempts, diet, D3 Regime tracking ect. Hope you all like it. https://github.com/MyDigitalFreedom/ClusterTracker/releases1 point
-
@dhuddly and to all reading. After a sleep I feel I overstepped with my comments above so I wanted to offer an apology and make clear that's my stuff, not his and I should have chosen my words better. Sorry Dhuddly, hope you may be able to accept my apology.1 point
-
We should also specifically look at adding video features. Because as I have learned recently, all of us talk and type differently. We are from all walks of life. If there's been misinterpreting due to text lengths and formats then video is an option to help us differentiate things like crazy or delicate. Because when anyone lands here, it means that they are finally vulnerable enough to be here. For example, in video you guys would see me talk fast. It's my nature. But in text forums like this, I write very long replies. Not because I am long and slow or delicate. Lol for me it's literally an ADHD thing that's never slowed me down. If storage is an issue for video features then there are plenty of avenues we can use or explore. It also would allow for a healthier community experience because anytime you have a face and voice to connect to the text it paints the whole picture. Just some food for thought.1 point
-
Craig no offense taken. And sorry if this comes across as defensive, I am aware of what you describe, I am also aware that I don't talk how I type and I don't type how I talk. I can understand why you are saying this to me but I would suggest maybe checking out some videos I made during covid. They have nothing to do with cluster headaches and only connect in a way that let's me know that the ch didnt take all of me and I survived. Beyond that the research I've compiled was a direct result of me fighting me way back so through the most traumatic and painful time in my life. I am described as a blunt person long before this. Through years of some of the same things you listed and can appreciate why you'd feel led to make sure I'm not out of my mind. I have no expectations from this forum. I am here because I needed to find community. People don't get through this level of trauma alone and sounds like you understand that. You can see those videos on TikTok. They've been there for years. I talk alot in them. The way you read my text in these forums will I guess allow you to understand that long responses, run-on sentences is kind of my thing. Even since MySpace I was aware that some people misunderstand how I type sentences in text. Just like this reply is too long. Its just something I've accepted decades ago. In person, I am the type that is comfortable delivering hard messages to people and that translates to caring. And that is definitely something we share Craig. Oddly enough, the first thing I did as far as treat myself to normalcy after ch was to write two books that I began back in the videos im talking about. Years of me being me brother. I have the grammar of a 10 year old and vocabulary of a truck driver. But that doesn't mean I'm out of my mind brother.1 point
-
Come chat with us! This is our annual virtual gathering where Bob Wold, members of the board, and members of our community gather to chat, learn, and just be together. Patients, care partners, supporters, and friends are all welcome https://us06web.zoom.us/meeting/register/jnmTEWaeQAela08Ij0PBTg
.thumb.png.1a9fe4b380e44c4016e23864c94d0ee7.png) 1 point
1 point -
See you there1 point
-
If we could compile a detailed list of what the app would need to do I could have us a fullstack app in no time. I can do several frameworks but enjoy NextJs the best since it is web based. No need for playstore and apple when you use NextJS. This website here is great though and could easily be converted. If you mean a native app, I would offer some positive pushback why keeping it web based can reach more people though. If you mean social media type of app with various functions and more dynamic than static, I have a couple MVP's collecting dust we could use. Whatever you decide though please know I'd definitely volunteer my skills and knowledge for the mission.1 point
-
80/day is very unlikely to benefit you, and I wouldn't hope for much from 160/day, either. (240/day is pretty much the most standard starting dose, increased over time as needed.) It seems that immediate release works better than extended release. Also, it takes time for verap to get into your system and help at all. Could be that your doc is starting with extreme caution for some good reason, of course. Often, a course of prednisone is recommended to at least hold off the pain while the verap is settling in. But, really, the D3 regimen is a better preventive for most people than verap, with a lot fewer potential side effects. (see attached) What else are you using for your CH now? You might want to look at this: Basic non-busting information - ClusterBuster Files - ClusterBusters. Also, I have attached an older summary of CH treatment options. It's old enough that it doesn't mention the newer CGRP drugs, but I think what's there is still mostly valid enough as a point of reference. Quick Start Guide - Sept 2023.pdf GoadsbyCluster.pdf1 point
-
What a great post. Thank you. I'm looking forward to perhaps a follow-up from @Craigo This seems possibly valid to me. I'm just wondering how you reached the conclusion, and why "undiagnosed." In Rozen's big 2011 study of people with CH, he asked about other medical conditions that people with CH have, but it doesn't seem that ADHD was among the possible answers. Someone at ClusterBusters might know whether another big study is planned (there was another one, after Rozen's, by Larry Schor), since CB is a source for research subjects. It seems like this is a question that might be asked (at least about diagnosed ADHD). Also, regarding dopamine, I admit to not having studied the two reports I posted in the research/scientific news section below, but I guess I could imagine that increased dopamine production accounts in part for the effect of D3 on mood.1 point
-
I'm not sure how a PPI would help for CHs. In fact, one of the common side effects is severe headaches. https://www.nyheadache.com/blog-posts/ppis-are-the-worst-but-all-heartburn-drugs-increase-the-risk-of-severe-headaches#:~:text=A new study just published,having migraines or severe headaches. "A new study just published in Neurology showed that people taking proton pump inhibitors (PPIs) such as omeprazole (Prilosec) and esomeprazole (Nexium) have a 70% higher risk of having migraines or severe headaches." I take rabeprazole, for GERD; but, started taking it after successfully busting. So, I can't say whether it has had any effect on my CHs. But, I just don't see how it would help.1 point
-
Your post hits me in the feels. It really does. I would say it is changing lives. I have had one of those days, your post is timely and let me be as real as I can with you on what is a topic that lies close to my heart. At least once, more often several times a week, I receive an email from someone who found www.vitamindregimen.com, come across Clusterbusters, a social site or watched one of the interviews with Pete Batcheller on YouTube. They rolled the dice on the regimen and got pain free. They write to say it changed their life. Even one of those emails is enough to justify every hour of advocacy. It’s worth it. I have spent over a decade now reading obsessively on this topic, not just to understand why and how the regimen may work, but to also understand why a percentage of people do not get fully pain free when applying it. Along the way I have interviewed some of the most amazing people in the vitamin D3 research space and with every interview, every study read, every question asked, I feel like I have moved a little closer to an answer and built upon my knowledge of the subject. I am so grateful Pete opened that door for me. That man is a global treasure. It’s also perplexing because this week alone I have seen cluster headache social media channels suggest ginger, purple cabbage, and today, chewing on a lime. I should have become a fruiterer! I understand the premise behind criticism of the regimen or pushing it to the side as a bunch of simple pills. From the outside, a handful of vitamins can look just as batshit crazy as cabbage when stacked against the sheer terror of CH. I get it. That is the real challenge. How do you communicate the regimen in a way that reaches more people, without overclaiming, without slipping into evangelism and without being lumped into the bucket of folk remedies? How do you communicate something that sits uncomfortably between patient-led discovery and clinical blind spots? I may have an opportunity to do more having just resigned my job today with no intention of continuing on the same path / career. 43, soon to be jobless - very tempting to study and see what further value I may add to this important body of work. Never too old right? Absolutely agree with you, happy for you to have found success with it and pleased to see you here on the CB forums!1 point
-
So true Jeeb. Unfortunately full and continuous cessation has yet to be achieved through the D3 regimen. Less frequent attacks, regular cycles and intensity of attacks has been greatfully experience from many on the regimen making it a very useful tool for any CH sufferes toolbox.1 point
-
@Nikkk I'll echo Craigs kudos for offering your time and skills!! I've lived long enough to become the elder statesman of the forum having been here since our go live date 16 years ago and counting!! That was Oct of 2009 and at that time the only online support sites were OUCH, clusterheadaches dot com which i think DJ launched in 1998.....and DJ was instrumental on getting us online as a yabb powered sister site. Although I've become the senior member, the jeebster AKA @Bejeeber and @CHfather got here in short order! I think Im safe in saying for all 3 of us that those years of the forum before Facebook were vastly different than they are today!! I've made several appeals at past conferences for folks that I personally know and who were once active members to take a little time and comeback and be a part of this community to no avail!! Although we transitioned to the current forum software probably 10 years ago, it is still a "static" type of board vs the "dynamics" of Facebook. As a result the forum has become just a few active members who support the few clusterheads who happen to find us before they find the many support groups on the "Book"! I was able to have a conversation with our fearless leader Bob at our Conference in Dallas this past September regarding the future of the forum.......I walked away from that conversation not anticipating any upgrades!! However, I can't speak for Bob and will definitely bring this thread to his attention!! The real tragedy is that this is the only place that you get reliable, time proven advice on the "clusterbusters protocol" while in the Facebook groups the term "busting" has become so bastardized that the information and advice is often worthless!! I used to keep my eye on those groups but eventually got tired of sounding like a broken record as I tried to offer correct information when I saw bullshit advice being given and finally just gave up posting there!! As to an app, although I've never used one, I know that there are several out there in use......in fact we had a member here several years ago that developed an app called "Nobism" if I'm remembering correctly......but I haven't heard anything about it either here or Facebook in at least a couple years! Once again, kudos and welcome to the community!!1 point






.png.3c8cd0ad8cddd8a0ba826717dc1ebdcd.png)
.thumb.jpg.24dde7ef3152d6d31b9546e3fec3b26d.jpg)

