
Bejeeber
-
Posts
5,193 -
Joined
-
Last visited
-
Days Won
403
Everything posted by Bejeeber
-
100% agreed here after decades of forum monitoring - between the two of us @jon019 we probably have going on 50 years of forum monitoring action.
-

where to fill oxygen tanks NewYork City with no insurance
Bejeeber replied to gracie's topic in General Board
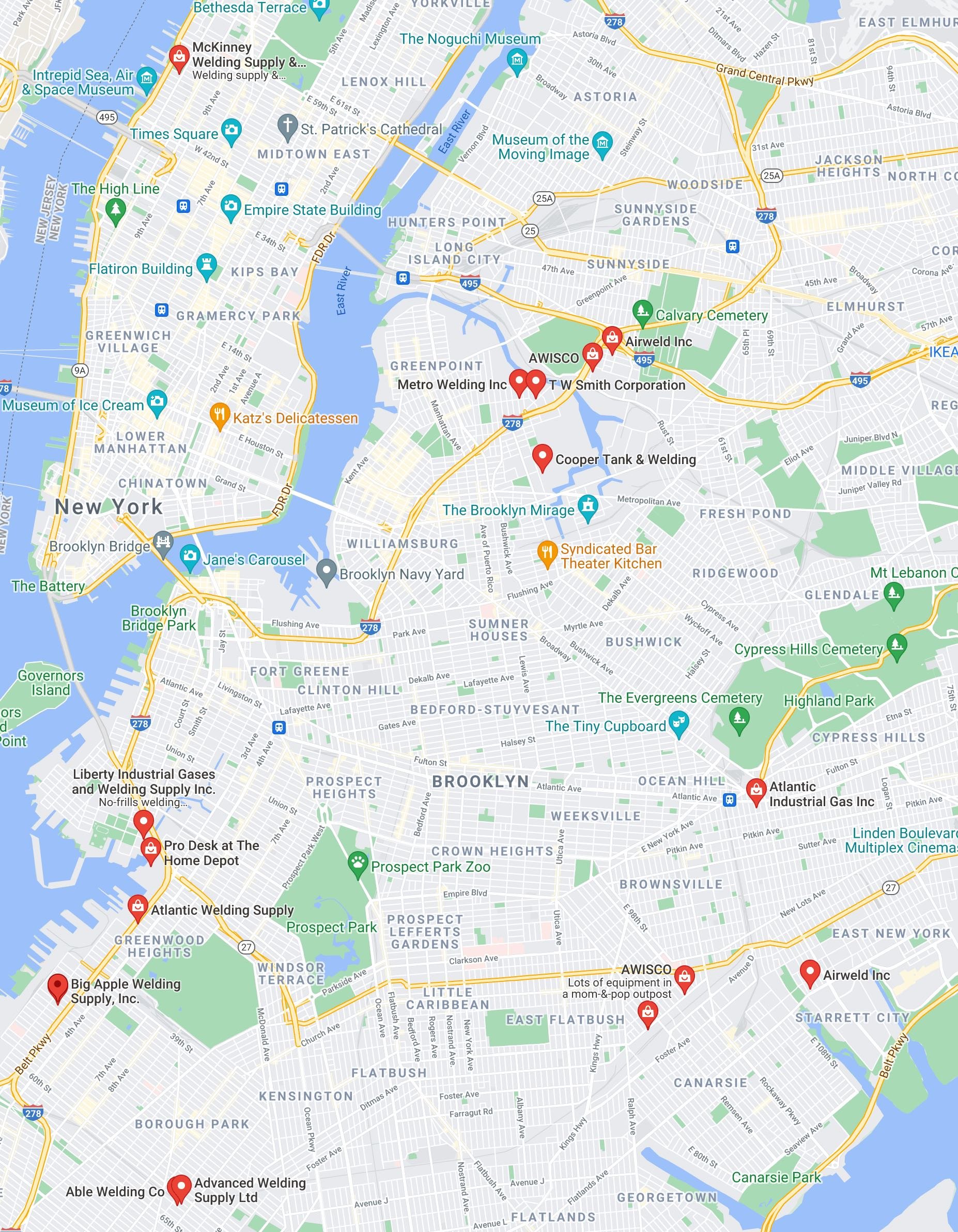
Until someone better acquainted with your dilemma pops along here, I'll just mention that when without insurance or prescription, lots of CH'ers have switched to using welding O2 (it is reputedly the same stuff). This was the result of my quick googling for "welding tanks delivery brooklyn", though I don't actually know whether any of these suppliers deliver like the medical O2 places generally do: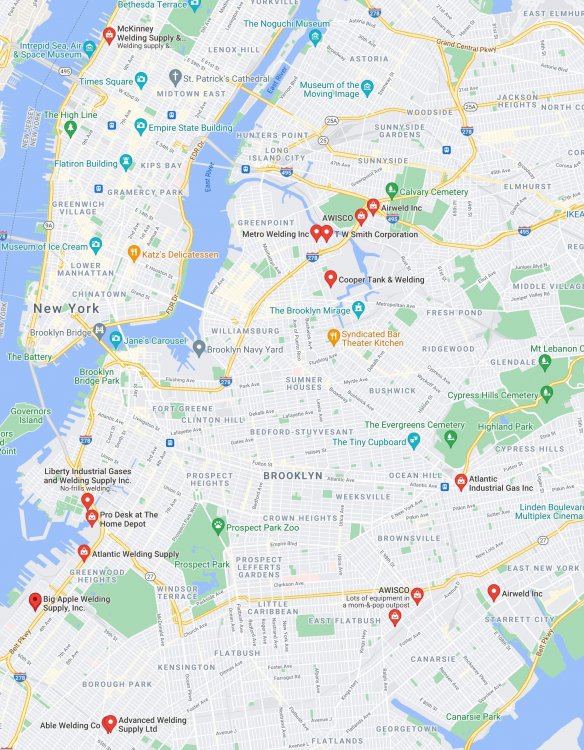
-
CHer with back pain, starting new preventative plan
Bejeeber replied to Amy123's topic in General Board
Other than the back thing @Amy123, your symptoms sure do sound classic, and very much like my experience, at least when I was "starting out". Yep, not just a neurologist, but a headache specialist neurologist is your ticket in the doctors dept. So many Ch'ers have been disappointed that a garden variety neurologist can be about as informed about CH as your GP is! You could consider seeking out a telemedicine appointment with an expert. You've probably seen that lot of CH'ers just scoot right around the roadblock of no access to medical O2 and get welding O2 (which is the same stuff) with no need for prescription. Maybe not as easy in a small town. That 6mg triptan you got (injection I presume) was actually 4mg too much. I've been shocked that I, like countless others, can routinely abort attacks (if caught at onset), with 2mg injections. Injections are the fastest, most effective way to abort with a triptan, and splitting doses into 2mg allotments sure helps con$erve supply and lessen side effect risk. I wouldn't recommend waiting until off of pred to start the D3 regimen, I think you should hop on it yesterday. If the D3 doesn't completely prevent your next cycle, busting very often can , and the combo of the two can pack a powerful anti-beast punch, but for best results you do wanna initiate the busting prior to when you expect the will beast pop back for a return visit. -
Glad to see you're getting such good advice on here Bosco. I'm going to agree with and comment further on a few of the recommendations: Yep, pred can indeed supply a couple weeks break, but one more thing to watch out for with it is that some of us find the CH can then come back with a vengeance. What looked like a D3 auto-response that you received may have actually been a personal response from the world's top expert on D3 regimen for clusters, if it came from "XXX". It is my impression that the CH'ers most successful at suppressing it, and often shutting it down for long periods of time - like years on end - have mostly abandoned the pharma for the very effective busting, etc. An energy shot will have that much less junk to consume in it than an energy drink. Topomax is pretty much universally reviled among those who have been on it, precisely for the cognitive hit you noted, not to mention its general ineffectiveness
-
My couple of Pfizer jabs (months ago) didn't kick up my episodic activity any.
-
I recall being shocked when first hearing of CH'ers experiencing a side switch, but I guess like many others, I've seen enough such reports that they provoke pretty much zero shock value any more, and even seem fairly common. Sorry to hear you went through that ordeal @kat_92 - if it was an MSG or similar food culprit, here's hoping it can be avoided easily enough going forward for prevention of a repeat. I could understand you becoming pretty gun shy about ingestion of soy sauce now!
-
Ah, searching the forum now and seeing how individuals such as our reality checking uber expert @CHfather have been keeping an eye on the nitrous and how one CH'ers abortive may be another's trigger with it.
-
Thanks Vipul!
-
Hi Vipul, would you be able to post the ingredients and their strengths (like 2x, 3x etc.) for the homeopathic meds you were given?
-
Wow, @spiny, clearly you've been through the epi ringer too, and have some seriously convincing evidence after those various procedures that points right at the epi being the culprit. I actually had the beloved colonoscopy without any sort of sedation or nothin', in order to avoid provoking any CH. Painful? Yes, but of course a relative walk in the park compared to Mr. You-Know-Beasty-Who.
-
Thank you for the cautionary tales @xBoss- that is some seriously messed up dentistry provoked hell. And @Ricardo, WOW, somehow I had missed or forgotten along the way the thing about laughing gas being an abortive???!!! I recall being given nitrous oxide as a grade school kid while getting some baby teeth molars removed, and man I was partying! I think it ended up being a serious inspiration for seeking out the party smokes when I could get access a couple years later.
-
So it sounds as if there's the chance with some of these dentist visit induced horrors that the dentist actually poked a trigeminal branch or something, but epi is generally the most likely suspect for pointing fingers of blame at. And I think it may just now be dawning on me what "keister a Zomig" implies.
-
Yikes you guys, udderly nightmarish on both accounts. @xBoss, when you got kicked out of remission, would this have been at a point in the cycle where alcohol consumption was still safe enough, but (confirming worst fears ) the epi packed that much more of a trigger punch?
-
Thank you for that highly pertinent report from the trenches Mr. jon! If I could knock out an epinephrine induced one off hit with a triptan while not triggering a cycle, I'd consider that a big win. It sounds like in your scenario that when you came to, the attack may have been well underway though, with no chance to catch it near onset.....
-
Like, if you're in a remission place where your ordinarily major trigger alcohol doesn't set you off, would epinephrine potentially be that much more still of a trigger than alcohol?
-
As I search 'epinephrine' here and on f-book I see practically all of the most respected CH advisors warning of what a major trigger it can be, and I'd really be a fool not to take those warnings very seriously! With some impending sinus surgery (just an outpatient deal, something I think of as being no big deal), the only real concern I have is the epinephrine factor. I'm inspired to ask if many other episodic CH'ers in remission have had the lidocaine/epinephrine stuff injected without being set off CH-wise? Apparently epinephrine is favored for its ability to discourage too much bleeding with procedures around the head area with all it's vascular pressure and fondness for shooting streams of blood out as if propelled from a device such as a Super Soaker™ squirt gun.
-
Sorry you are having such a rough go with the CH Eli, but glad that some of the best, most qualified advisors possible have been weighing in here so far. From this it sounds like if you were to keep up with the alternative therapy (busting?) every couple months, you could go into some genuinely long term remission, as many before you have? Although personally of the male gender, I have long suspected that the refusal of so many doctors to diagnose females with CH has been based on a self perpetuating medical myth that it is so much more prevalent in males. If you are continuing to use imitrex, one strategy you could consider would be to have a lower dose syringe pre-loaded and ready to go so there wouldn't be any real thinking or calculating required when you need it to administer it. This would probably require being well rehearsed with exactly what you would do when the time came, and this rehearsal could be done at a time when you are not actually having an attack. I have been there and done that. Markings of (2mg) doses on the syringes, and a plan for super easy, painless subcutaneous injection in the abdomen were part of the preparation process.
-
Chronic clusterheads... how do you know when a new hit starts?
Bejeeber replied to trjonas's topic in General Board
As a fairly textbook episodic CH'er I can say that once an attack has gotten a real foothold I've never been able to knock one back with O2 It's more of a catch it at onset or forget about it deal, so I feel like I understand where you're coming from @trjonas with not being able to tell if O2 would be of any use, since your onset was months ago! -
Hi ifb, glad to see you got the super expert advice from CHf! sucking ice cubes (especially when placed on the CH side of the roof of the mouth) has worked for me as a helper for aborting attacks when I'm not in in a high raging phase of a cycle, but it's been an adjunct when also breathing freezing cold air at the very first sign of an attack. In warm weather this can be done by going out to the car (if you have one), blasting the A/C, sticking your shnozzola up the the vent, and doing some serious nose breathing. Then around the time a gloriously delightful in comparison ice cream type headache kicks in, the attack may just be aborted. And hey the ice cubes might even work in conjunction with the O2. I'm not familiar with Cambia, but if that's all ya got, one trick others have used with some success with oral versions of triptans - which take a while to kick in - is to take it right before sleep, if you get the typical wake up hit about one hour after falling asleep. A funny phenomenon some of us have experienced is we can throw back an energy shot (like the 5 hour brand) or drink (like Red Bull) to help abort a hit, then go right back to sleep. I'd say your doc was actually correct about the Zomig at the beginning, not during. You'll encounter numerous headbangers here who have knocked out entire cycles via the busting that CHf mentioned, and many who report good results with the D3 regimen.
-
Happy and successful busting to you xBoss. May the bust abide indeed - good one jon.
-
WTH!! Essential Oils worked?!! (Edit - not really)
Bejeeber replied to tmac's topic in General Board
Intriguing stuff, tmac, I'll be following your updates with interest. -
Washington Post article (4/3/21) featuring Bob Wold and Clusterbusters
Bejeeber replied to MaxHead's topic in General Board
Ooh, thanks for the tip off, I read it and liked it - a bit surprised my Google News feed hadn't offered it up already, as it tends to know (after I've allowed it to spy on me) that I'm interested in this sorta thang. -
Hi cgold! I'm afraid your story of being brushed off and misdiagnosed as a female is one I've noticed others reporting all too often. Sometimes makes me wonder if CH really is more prevalent in males, or if doctors are still just stubbornly continuing to refuse to diagnose females based on a myth. Last I checked, 7 weeks is nowhere near what is considered the chronic zone, you'd have to go on continuously for many many months (I think it is n the neighborhood of over 6 months, maybe someone can come on here and remind me), to be edging towards a chronic classification. Personally as an episodic I can say that yes over the decades the cycles and duration of attacks have steadily gotten longer and the pain has intensified. What first started as 2 weeks of attacks maybe once a day, a half hour each, very gradually devolved into 2.5 month long cycles, several attacks a day, and if an unaborted one breaks through it can go on 3-4 hours. BUT I still count myself lucky, as the remissions have also accordingly stretched out longer and longer. Many blame things like imitrex use for worsening their cycles. I don't particularly doubt them, but my CH went ahead and started continually worsening before imitrex was even available in the US. I like all the stuff FunTimes has mentioned, plus you'll find lots of talk about "busting" over on the Share Your Busting Stories forum where busting is discussed by registered members. It's not really discussed here on the General Board, but this is a quick indicator of what it is about, pasted from the Treatment Options and Choices for Cluster Headache Patients public section of this Clusterbusters site: Fast Statistics on Cluster Headache and Indoleamine Hallucinogens A 2006 study conducted at Harvard Medical School found remarkable results in CH patients and LSD or psilocybin mushrooms: Psilocybin reports: 22 of 26 patients said psilocybin aborted their attacks. 25 of 48 patients said cluster cycle was terminated. 18 of 19 patients said psilocybin extended their remission periods. LSD reports: 7 of 8 patients reported LSD terminated cluster cycle. 4 of 5 patients said LSD extended remission periods. A 2017 qualitative thematic analysis of user accounts in forum discussions found: CH patients consider illegal psychoactive substances as a last resort. There is little to no interest in the psychoactive impact of these compounds. Patients choose sub-psychoactive doses to avoid or limit the “trip” effect. Patients reported prophylactic and acute treatment for cluster headache using psychedelic tryptamines: LSD and psilocybin mushrooms.
-
A lot of episodics such as myself return to normal life, with triggers not an issue, unless we're feeling some indications (like shadows) that the CH is lurking again and ready to pounce. I won't presume to speak for otherwise chronic clusterheads who have busted out of it though.